Health improvement is an objective of all economic-level countries to increase the well-being of populations and reduce mortality. A key indicator of population health is life expectancy at birth which offers a clear picture of how effective health interventions work and reflects the quality of life in a society. As healthcare innovations continue to progress, people are living longer, but not everyone benefits equally; health disparities are critical, especially in developing regions. In this context, we will examine the relationship between economic factors, such as GDP per capita and social contributions, and health outcomes in the Gulf Cooperation Council (GCC) and Levant countries. We will explore how economic growth affects life expectancy as well as mortality rates to find effective public health strategies in these regions.
Economic Disparities and Health Challenges in the GCC and Levant
The connection between economic prosperity and health outcomes is evident in the GCC and Levant regions, but countries with lower economic standing face more significant challenges. Qatar, with the highest estimated per capita income at $69,034 by 2057, could benefit from better healthcare, longer life expectancy, and overall improved health. On the other hand, the majority of Levant countries, including Jordan, Lebanon, and Syria, struggle because of limited economic resources. While Oman is a GCC country, it also faces economic constraints that impact health financing. By 2065, all these countries are expected to have some of the lowest GDP per capita and net income levels, which will directly affect their healthcare systems and public health outcomes.
The primary issue in these lower-income countries is the insufficient health expenditure, which limits the development of healthcare resources and infrastructure and result in poor health outcomes like higher mortality rates and lower life expectancy. Jordan, Lebanon, and Syria are known for having the lowest health expenditures in the region, with Oman’s spending relatively lower than wealthier Gulf countries like Qatar and the UAE. This creates a vicious cycle and consequences are unavoidably negative: limited funding results in fewer healthcare resources, which in turn leads to poor health outcomes. Countries with high mortality rates, like Syria, Oman, Lebanon, and Jordan, are therefore, resulting in health disparities.
These countries also have difficulty controlling social determinants of health, like education, income inequality, and access to basic services. They will continue to have disparities in health outcomes compared to their prosperous neighbors in the GCC unless a holistic solution is found. Mortality rates in Syria, Lebanon, and Jordan are high as they are struggling with the worst figures in the region. Additionally, life expectancy is lower in Levant Countries and Oman. Economic limitations are thus restricting health improvements and contributing to these disparities.
A Multifaceted Approach to Health Improvement
The current situation in these nations presents a challenge and an opportunity to develop strategies that tackle the root causes of poor health outcomes. A multifaceted approach should be implemented to overcome economic and healthcare system limitations.
Increased Health Expenditure: The most urgent step is to increase public health funding, as healthcare is critical for the Levant countries. This sector should become a part of the principal national budget. Innovative financing projects like collaborations or expansions of public and private health insurance should be considered, and funds from other sectors should be used differently. For example, the Quality of Life Programme in Saudi Arabia, which is in line with Vision 2030, aims to improve well-being and increase life expectancy to 80 years by that year. Public health is also given top priority in the UAE’s National Strategy for Wellbeing 2031, which encourages physical activity and healthy lifestyles while guaranteeing that the elderly population has access to better medical care.
Economic Diversification: Jordan, Lebanon, Syria, and Oman can work toward economic diversification to generate more tax revenue, which, in turn, could be reinvested into the healthcare system. Take the example of the partnership between Sharjah Research Technology & Innovation Park (SRTIP) and Deep Knowledge Analytics. They invest in biotech, pharmaceutical, and AI-driven healthcare sectors to stimulate economic growth while improving healthcare accessibility.
International Support and Partnerships: Levant countries also have the option to look for international collaborations, foreign aid, and grants to enhance their healthcare systems. Countries like Germany, which contributes the most to social contributions, have strong social safety nets. Utilizing these international resources can help in closing the economic gap between more developed and less developed countries. In the UAE, there is the Abu Dhabi Stem Cell Center (ADSCC) and the Omics Centre of Excellence, that can help Levant countries by dealing with health challenges like chronic diseases and facilitating knowledge transfer, and healthcare innovation.
Focus on Preventive Care: A shift toward preventive healthcare, including public health campaigns, immunization programs, and lifestyle changes, is essential. Currently, GCC countries focus on longevity programs that deal with critical lifestyle factors affecting health outcomes, such as diet, physical activity, and nicotine use. Initiatives such as displaying calorie counts on restaurant menus, imposing sugar taxes on sweet drinks, and launching educational programs that promote healthy eating and active living could be implemented in Levant countries, hence reducing the risk of chronic diseases.
Social Determinants of Health: Prioritizing education, fair income distribution, and access to sanitary facilities and clear water are all critical for improved health. Better health outcomes and an overall higher quality of life will result from this.
In conclusion, there is a strong correlation between health disparities between GCC and Levant countries and economic factors such as GDP per capita, income inequality, and healthcare expenditures. Many Levant countries still have low incomes and insufficient healthcare investment, but GCC countries, especially Qatar, have high-income levels and better healthcare outcomes. Therefore, some recommendations are related to economic diversification, and social determinants improvement to break the cycle of poor health outcomes and reduce the mortality gap. These actions can maximize life expectancy and build a healthier future for the entire region.
Srtip. (2024, September 10). Sharjah Research, Technology, and Innovation Park showcases innovations in vertical farming at the global vertical farming show 2024. Sharjah Research, Technology, and Innovation Park Showcases Innovations in Vertical Farming at the Global Vertical Farming Show 2024. https://blog.srtip.ae/srtip-showcases-innovations
In the intricate tapestry of a nation’s prosperity, nothing weaves a more profound impact than the state of its healthcare system. The vitality of its citizens, the resilience of its communities, and the promise of a prosperous future all hinge on the health and wellness of the population. A healthy population is a productive one, as it reduces absenteeism, increases workforce efficiency, and stimulates economic growth.
Yet, as we embark on this journey through the labyrinth of healthcare, one question looms above all: How can we chart the course to assess and improve a country’s medical system, ensuring a brighter, healthier tomorrow for all? Evaluating the medical system of a nation is a complex endeavor that requires a comprehensive approach to several factors we will delve deeper into later.
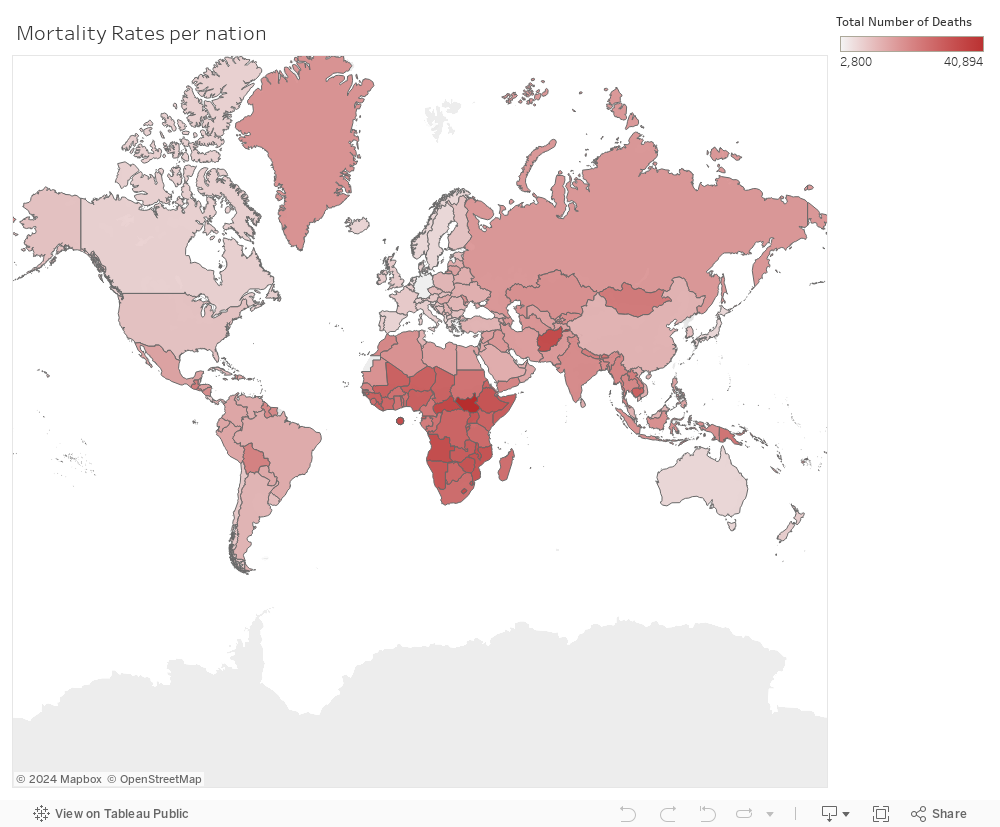
One indicator that may be used to assess the effectiveness of the medical industry is the mortality rate. From the data provided by World Development Index, countries with high death rates, such as the Central African Republic, Niger, South Sudan, and many others, have poor healthcare systems, as seen in the visual below:
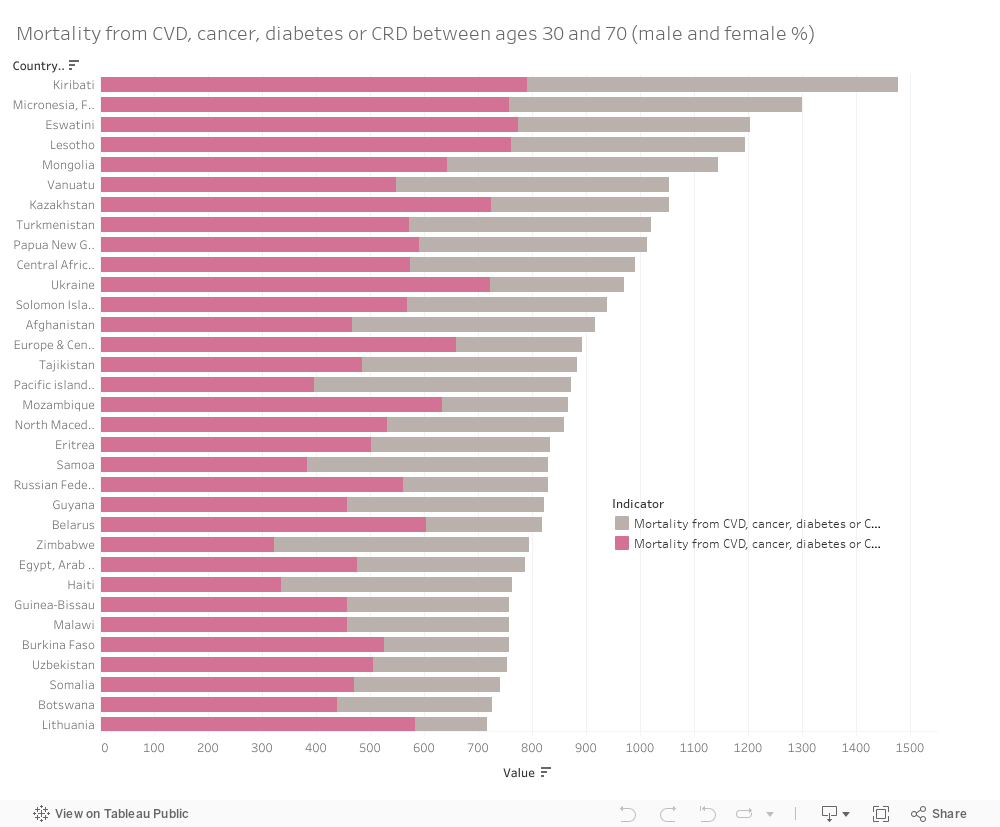
Furthermore, there exists a strong correlation between CVDs, cancer, diabetes and other illnesses that significantly impacted the mortality rate indication for both males and females. This implies that countries experience high mortality rates due to the increasing rates of the above-mentioned illnesses and diseases. Also, an implication of the absence of some healthcare services such as a lack of efficient medical professionals may be valid as well in such a case.
As a matter of fact, the presence of medical professionals that can assist society and offer health care is one of the most important measures of how well the medical sector is doing. Therefore, one potential solution is enhancing the availability of medical professionals that are prone to doing their job effectively.
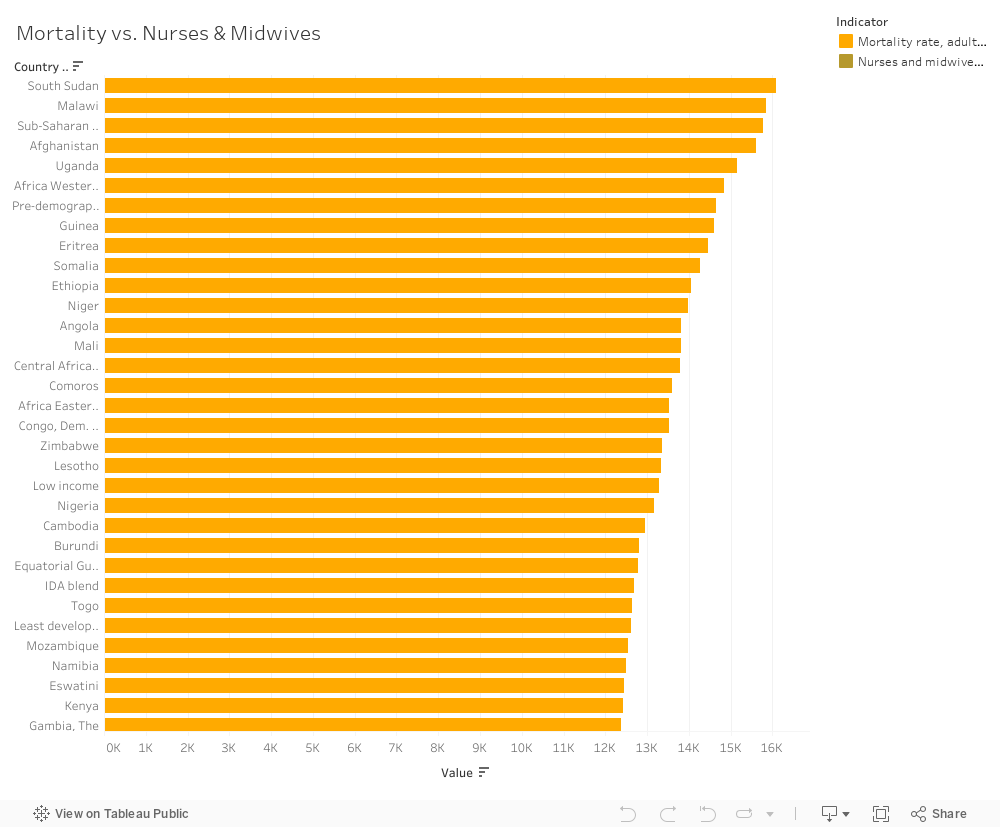
There exists a weak correlation between the availability of nurses and midwives and the increasing rates of mortality. This is because an effective team of well-experienced nurses and midwives can strongly lead to a decrease in the number of deaths per hospital. The top 5 nations with the highest mortality rates also have the lowest number of nurses and midwives.
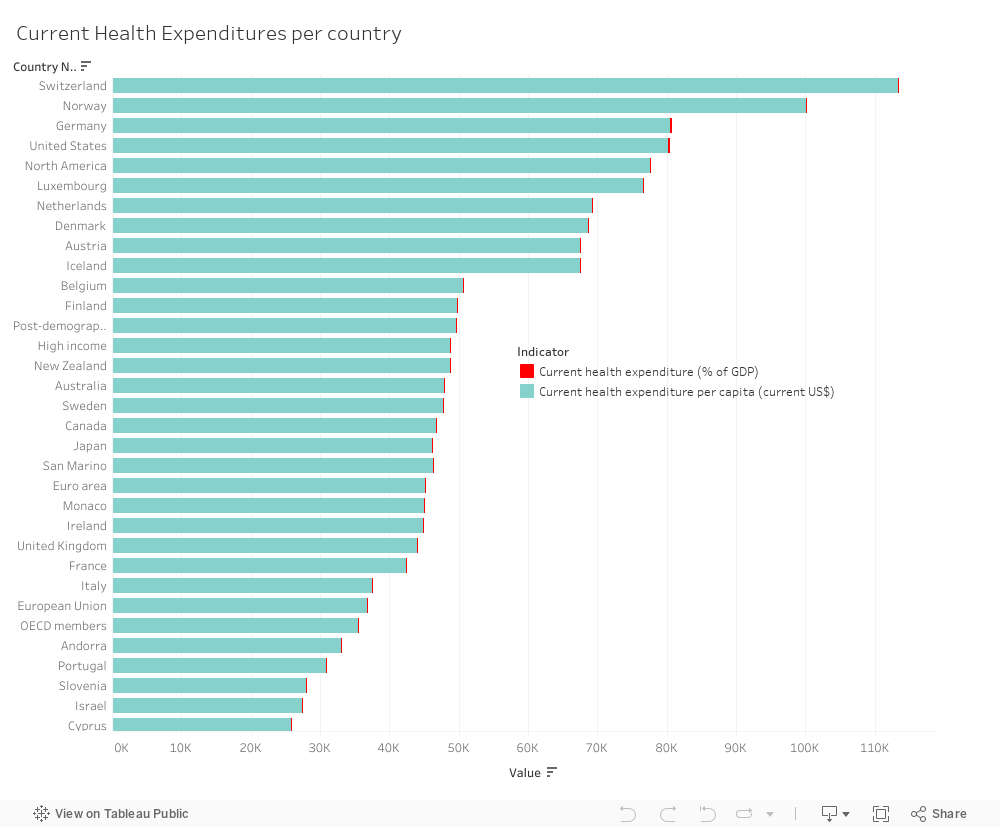
Another potential solution involves increasing expenditures in the healthcare field to gain access to more promising and efficient results. In order to improve the health of their medical industry, the nations with greater rates of mortality have to gain insight from the experience of those with developed healthcare systems, where a significant percentage of the more developed countries’ expenses goes to health expenditures (ex: United States, Denmark, Luxembourg, Norway etc.) Higher expenditure on healthcare implies higher expenditure on more enhanced medical professionals whose primary role is to save the day by decreasing mortality rates. Moreover, we can see that while less developed nations such as South Sudan and many others have far greater mortality rates (as discussed earlier), they almost all have a lower number of health expenditures too.
Countries with high mortality rates should prioritize expanding their nurse and midwife workforce. This can be achieved through targeted recruitment, better training opportunities, and incentives to retain experienced healthcare professionals. In nations with a scarcity of healthcare workers, it is crucial to consider redistributing them from regions with surplus staff to areas with greater need. This can help ensure more equitable access to healthcare services and reduce mortality disparities.
Also, the observation that less developed nations with higher mortality rates also have lower health expenditures highlights the need for increased investment in healthcare infrastructure, training, and resources. Adequate funding can have a significant impact on healthcare accessibility and quality.
In conclusion, the state of a nation’s healthcare system is a complex web created by several kinds of variables. According to the results of our investigation, nurses and midwives are vital in determining healthcare outcomes, and there seems to be a link between their availability and death rates. Key suggestions to improve patient care and results included strengthening the healthcare workforce through recruiting, skill development, and equitable distribution.
Furthermore, the evidence indicated a clear link between less health expenditures and higher mortality rates in several less developed nations. This emphasizes the urgent need for increased funding and resources to bridge healthcare disparities and improve the well-being of vulnerable populations.
As we journey towards a brighter future, let us remember that the path to a thriving medical system lies in unity, innovation, and data-informed decision-making.
FROM “Man up, you can’t be depressed just because this happened!” TO “Why are you looking so sad and tired? Are you depressed? You can talk to me if you want..”
To begin with, according to the World Bank dataset on development indicators, it is clear that men’s average suicide mortality rate is significantly higher than females.
Surprisingly, males are three times more suicidal than females, reaching an average of 14.3 male suicides per 100,000 males, while 4.4 female suicides per 100,000 females.
But why is this the case?
While comparing countries with high unemployment rates and countries with low unemployment rates, the following analyses were investigated:
To begin with, in Countries with highest unemployment rates, the suicide mortality rates for both men and women are higher.
However, when faced with difficult economic situations:
Females suicide mortality rates were higher by 150%
Males suicide mortality rates were higher by 217%
This leads to the conclusion that men’s mental health tends to be more susceptible to financial burdens.
So, what should be done?
A potential solution would be providing unemployment benefits, which are governmental compensations that are provided for unemployed people. These compensations help secure a stable income after the layoff of an employee, and they improve unemployed people’s productivity in the labor market by improving job matching and connecting employees to employers.
In addition, this solution can be helpful in mitigating the impact of unemployment on the psychological wellbeing of people.
As the following illustration shows, both females’ and males’ suicide mortality rates are higher in countries with loweradequacy and coverage of unemployment benefits
More specifically, males’ suicide rates are 31% lower in countries with high adequacy and coverage of unemployment benefits.
Thus, in order to mitigate the males’ suicide mortality, several recommendations are suggested to be effective.
First, it is highly recommended that suicide prevention groups intensify their focus on men and encourage them to express themselves and seek psychological help.
Equally important, in countries with high unemployment rates, governments should work on providing unemployment benefits and ensure their wide coverage of the unemployed.
Accommodating the Covid-19 Sick Patients within Hospital Beds has been the main challenge worldwide for poor and rich countries alike and for countries with strong healthcare systems and weak healthcare systems alike. Securing these beds is a life or death situation for the Covid-19 critically ill patients who need special intensive care beds. This visulaization will show you the distribution of intensive care patients by country and will show you that the more hospital beds available per 1,000 poulation the lower the Covid-10 mortalility rates.
As per the scatter diagram, countries with higher number of beds per 1,000 population have maintained lower Covid-19 mortality rate even after they went into the peak of Covid-19; best example being Japan with only 4 dead per 1 million population. This is contrasted with England for example which, even prior to reaching the peak of Covid-19, had a high Covid-19 mortality rate of 305 per million. In Japan, there are 13.4 beds per 1000 population whereas in England there are only 2.8 beds per 1000 population.
As per the heat map, we find that Brazil, Iran, Vietnam and Thailand are having the highest percent of critical care patients. Also, this map shows that Lebanon has a 6.53% of critical Covid-19 cases.
As the World is today coping with the new virus COVID-19 that spread five months ago, leading to millions of deaths behind, it has been proven that health is the most important component on the human life, and that the existence of advanced, progressive and up to date health care and health centers are crucial for an efficient health assistance for a whole given nation. As such, I found in the World bank dataset some indicators that were efficient enough to picture the correlation between health expenditures and the lifetime of infants and adults.
We can spot how health expenditure per capita varies from region to region, leaving a considerable influence on life expectancy. In fact, Europe, that has the highest health expenditure(1,200,000 $), has the highest life expectancy recording 77 years. Africa that has 61,347$ expenditures, expects an average age for its population equal to 56 years. This is very logical since the absence of social welfare, health care, and the limited number of sanitarian and health centers prevents ill people from having their medical treatments’ needs, which therefore leads to their death. However, a third indicator was included which is the infant mortality rate that has a negative relationship with the health expenditure. We can notice that Europe has the lowest rate 0.7% compared to Africa that has 6.7% mortality rate among infants. Thus, we can conclude that Europe which has the highest health expenditures has the lowest infants mortality rate because of the provision of vaccinations, and frequent followups with doctors. Whereas, in Africa, where there are a lot of diseases, there is lack of medical personnel and machinery used to assess and diagnose ill children, or infected pregnant women.
Thus, the integration of technology in health and sanitarian sector and the presence of social welfare and well-prepared medical centers proved to have a positive relationship with the health and the lifetime of people, including children.








 While comparing countries with high unemployment rates and countries with low unemployment rates, the following analyses were investigated:
While comparing countries with high unemployment rates and countries with low unemployment rates, the following analyses were investigated:




