by zct01 | Nov 21, 2025 | Uncategorized
A Morning in Akkar
Somewhere in the hills of Akkar, a mother wakes before dawn. Her son is burning with fever, his tiny chest rising in short, frightened breaths.
She wraps him in a blanket, steps outside and faces the same impossible truth every family in her town lives with:
There is no clinic here.
No doctor.
No nearby care.
The closest medical help is more than an hour away—if roads are clear, if transportation can be found, if nothing goes wrong. For her, and for nearly half of Lebanon’s towns, simple illnesses can become life-threatening journeys. It is not just a healthcare issue, It is a daily, silent tragedy that shapes entire lives.
What the Data Shows but the Country Ignores
The visuals map this tragedy with painful clarity.
In the bar chart:
-
49.74% of Lebanese towns have no local resources nor nearby healthcare.
-
17.08% have no local facilities but can sometimes reach distant care.
Only 33.19% enjoy the basic dignity of accessible treatment.
The map shows Lebanon carved into colors that reveal the geography of abandonment.
-
Akkar, North Lebanon, Baalbek-Hermel, and Bekaa glow in urgent shades of red.
-
Beirut and Mount Lebanon rest confidently in green.
-
Though South Lebanon contains the highest danger percentage, it is covered with governorates that contain abundant amount of medical facilities and resources.
The visuals prove what families in rural regions already know: healthcare access in Lebanon is not just unequal—it is deeply, structurally unfair.
The danger zones are not random, they follow the borders of poverty, neglect, and distance.
A Country at a Crossroads
Yet Lebanon is not without hope. Around the world—and even within its own borders—innovative models show that remote and underserved communities can receive consistent care. The country stands at a crossroads where solutions are known, feasible, and within reach.
Lebanon can choose a future where no mother must gamble with her child’s life because of distance.
That future begins with a hybrid healthcare access model designed for real Lebanese terrain, real Lebanese families, and real Lebanese limitations.
Building the Path Forward
The path unfolds in two phases—immediate relief and lasting transformation.
Immediate Relief
-
Mobile clinics traveling weekly into remote towns.
-
Telehealth services connecting residents with doctors online.
-
Community health workers offering first aid, monitoring chronic diseases, and stabilizing emergencies.
These solutions bring healthcare to the people, rather than asking the people to chase it.
Long-Term Transformation
-
Expanding rural Primary Healthcare Centers (PHCs) in governorates painted red in the danger map.
-
Incentivizing private and nonprofit partnerships to open satellite clinics.
-
Improving transportation links so that even without a local clinic, emergency care is reachable.
This approach does not just fill gaps, it builds a system where every town becomes medically reachable, no matter how far, no matter how rural.
Why This Will Work
Proof already exists.
Organizations like MSF, the Lebanese Red Cross, and multiple NGOs have successfully delivered mobile and remote care across Lebanon’s hardest-to-reach regions. Telehealth has grown worldwide, saving millions in rural communities and the data that drives these charts, maps, and analyses pinpoint exactly where interventions must be prioritized.
The strategy aligns with Lebanon’s national health vision and mirrors international best practices in countries with similar geography and instability.
It is not theory.
It is tested, validated, and realistic.
Beyond the Diagnosis
The visuals do not simply highlight shortages, they illuminate where change must begin.
The Truth
-
Lebanon’s healthcare inequality is regional and predictable, not accidental.
-
Rural northern and eastern regions are in critical danger, lacking both local and nearby care.
-
Nearly half of Lebanese towns face severe accessibility barriers.
The Solution
-
Deploy mobile and telehealth clinics immediately to stabilize high-danger governorates.
-
Invest in long-term PHC expansion to ensure durable access.
-
Integrate transportation and healthcare planning, recognizing that distance is often deadlier than disease.
-
Maintain data-driven monitoring to continuously reallocate resources to evolving needs.
If Lebanon acts now and not later, the red zones can fade. Families can breathe easier. Lives can be saved.
A Different Dawn
One day, perhaps, a child in Akkar will still wake before dawn—but instead of gasping for breath, he will leap from bed to greet a new school day. His mother will no longer fear the distance to care.
Because care will finally be within reach. Because the map will no longer define who survives and who struggles. Because Lebanon will have remembered its forgotten towns.
That is the story the data tells. That is the story this country can still rewrite.
“We are alive the most when we are faced with adversity like no other.”

by nha59 | Nov 18, 2025 | Uncategorized
Access to healthcare in Lebanon depends on one simple but critical factor: where you live.
But until you visualize the distribution of facilities across the country, it’s hard to truly see how unequal that access is.
I started this project by aggregating six types of health facilities — hospitals, clinics, medical centers, pharmacies, labs and radiology centers, and first-aid centers — across all districts using the PKGCube Health Resources dataset. After cleaning and restructuring the data, one pattern immediately stood out: Lebanon’s map of healthcare is far from balanced.
To understand this more clearly, I built a district-level visualization and redesigned it using explanatory design principles. And once the noise was removed, the picture became unmistakable.
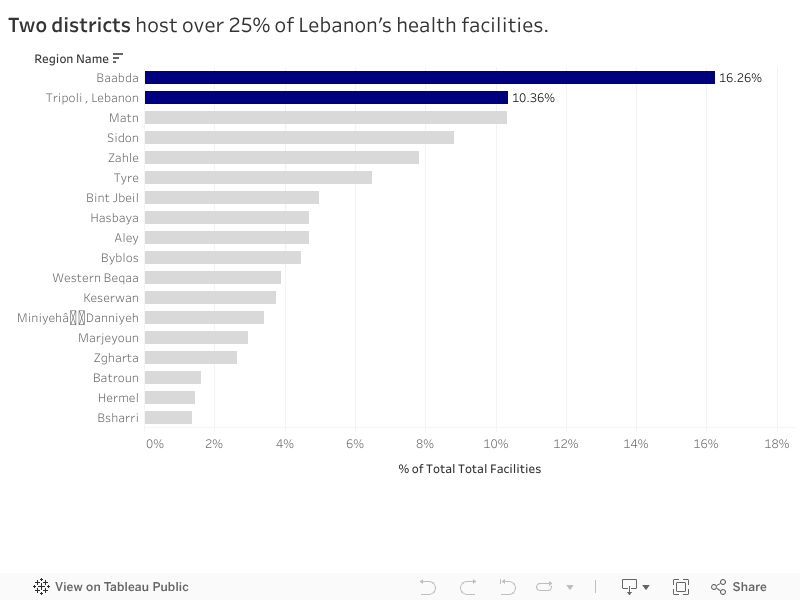
The Key Insight
Two districts — Baabda and Tripoli — hold more than a quarter of all health facilities in the entire country.
Just two.
Meanwhile, at the opposite end, districts like Hermel and Bsharri combined account for less than 3%.
In a country with major infrastructure gaps and uneven population distribution, this imbalance has consequences:
-
It shapes how far people travel to access care.
-
It affects waiting times, congestion, and referral patterns.
-
And in crisis situations, it determines who gets help quickly and who doesn’t.
The redesigned visualization highlights this story intentionally. The top two districts are shown in strong blue, while the rest of the country fades into context. No clutter, no distractions — the contrast lets the insight speak for itself.
What It Means
This distribution doesn’t automatically mean Baabda and Tripoli are “over-resourced” or that Hermel and Bsharri are “neglected.” Counts are not the same as capacity, staffing, or service quality.
But the numbers do reveal something important: If health planning is meant to be equitable, we can’t treat all districts as if they start from the same baseline.
Policymakers and NGOs could use these insights to:
-
Prioritize new facility investment in low-share districts
-
Support underserved areas with mobile clinics or telehealth units
-
Track whether the distribution becomes more or less concentrated over time
What Comes Next
This visualization is a starting point. The next step is to connect the facility distribution with:
-
District-level population
-
Accessibility and travel time
-
Facility capacity indicators
That is when the story becomes more than a map — it becomes a tool for planning.
For now, the message is simple:
Lebanon’s health infrastructure is unevenly distributed, and two districts carry a disproportionate share of the country’s access.

by aed05 | Nov 20, 2023 | Dashboard, Visualization
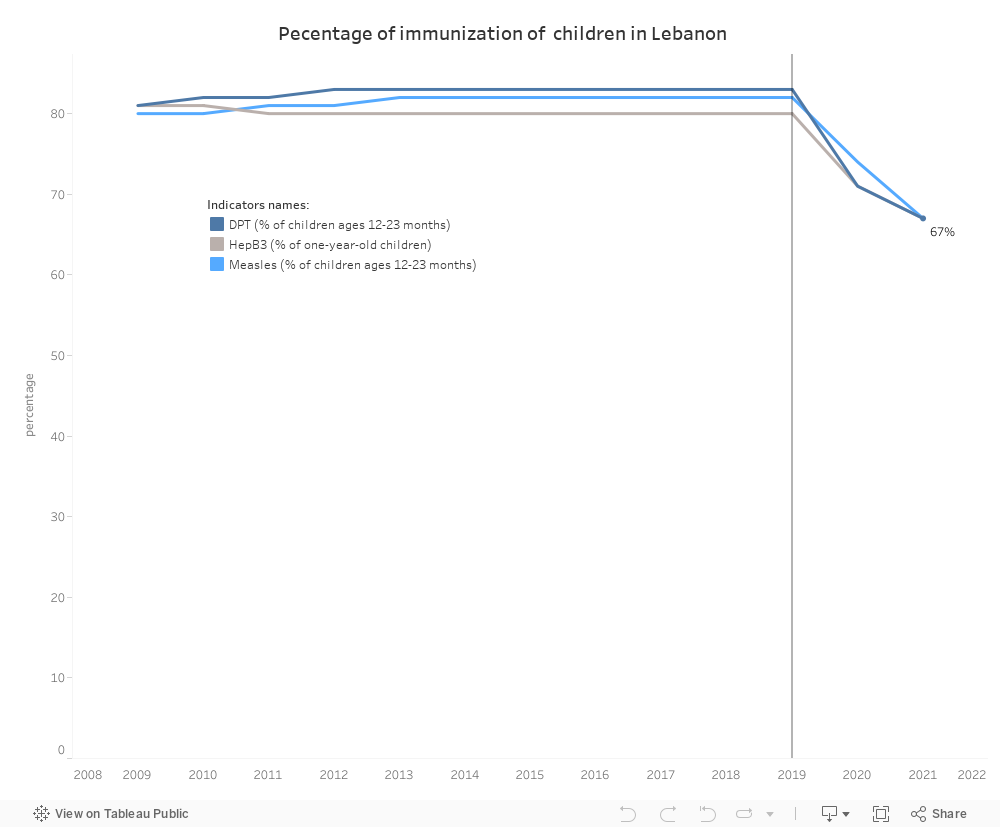
In 2020, Lebanon witnessed a substantial decrease in the percentage of immunization against Diphtheria, Pertussis, and Tetanus (DPT), Hepatitis B (HepB3), and measles among children aged 12-23 months. After more than ten years of stability, the immunization rate dropped to 67% in 2021, marking its lowest point in recent history.
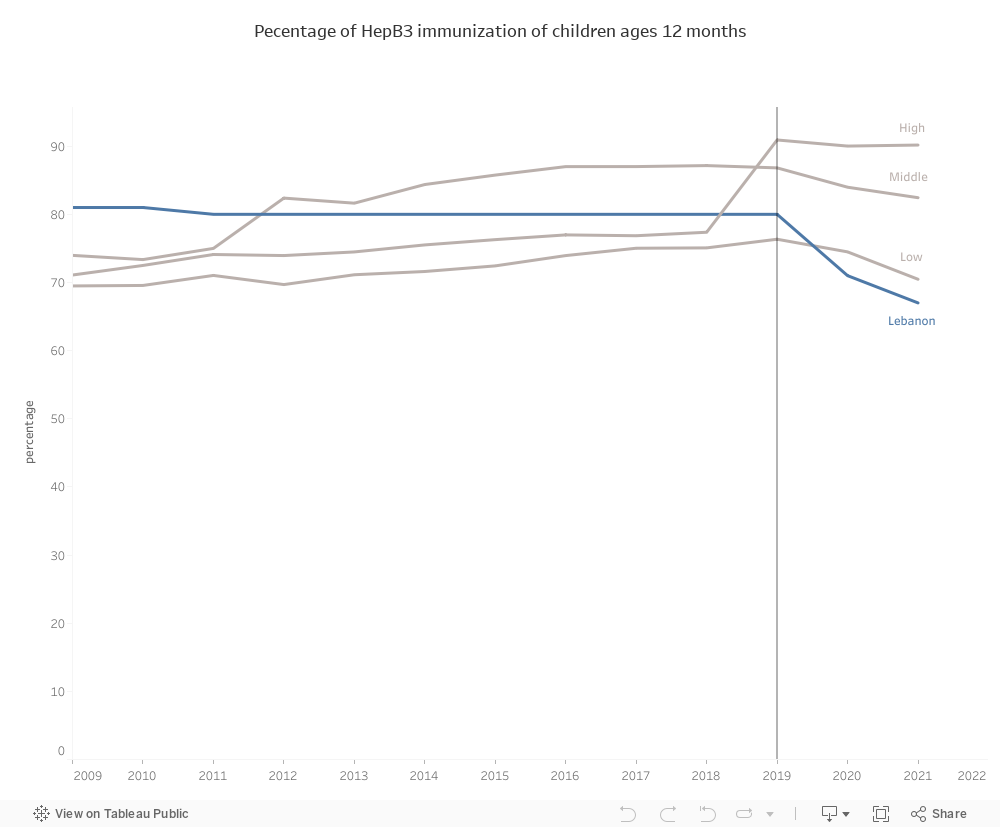
Standing Out in a Global Context of Decline:
While middle-income and low-income countries experienced a decrease in immunization percentages in 2019 and 2020, Lebanon stood out with the most significant decline. Comparatively, when pitted against low-income, middle-income, and high-income countries, Lebanon witnessed the highest decrease in the percentages of DPT, Measles, and HepB3 immunization during these pivotal years.
This raises crucial questions about the specific factors contributing to Lebanon’s distinct challenges in maintaining essential childhood vaccination rates.
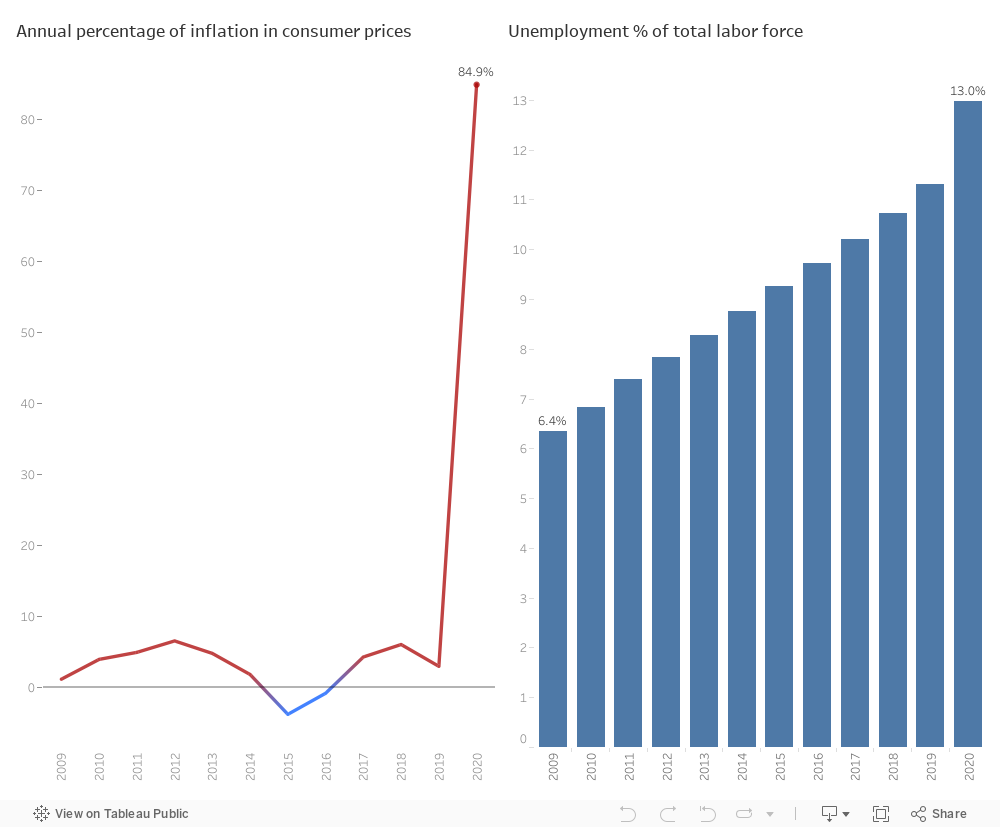
Economic Struggles Impacting children Immunization:
In 2019, Lebanon experienced a significant economic crisis, resulting in widespread job losses, with the unemployment rate reaching 13% by 2020. The cost of everyday items surged, approximately 85%, creating substantial challenges for individuals to afford medical expenses and seek necessary healthcare. Accessing healthcare has now become a luxury for many citizens, including children, as parents prioritize essential goods over vaccinations for their kids.
In addition, the Lebanese government allocated similar resources in Lebanese Lira to its healthcare system in 2019 and 2020 as it did in 2018. However, the impact of inflation eroded the purchasing power, diminishing the effectiveness of the government’s support, especially given that healthcare costs are often priced in US dollars.
Shielding the Health of the Lebanese :
In the world public health, the ramifications of low vaccination rates against DPT , Measles and HepB3 are far-reaching and dire. The repercussions extend from the heightened risk of individual health issues to the vulnerability of entire communities facing outbreaks. These outbreaks not only strain healthcare systems but also impose a substantial economic burden, creating a global health threat. The gravity of these consequences becomes most evident in the specter of preventable deaths looming over communities.
Recognizing the gravity of these consequences, urgent action is essential. The government must increase its investment in vaccination programs, ensuring free and universal accessibility. It should collaborate with international entities such as World Health Organization and NGOs to get financial support.
These efforts will not only promote individual well-being but also strengthen the communal defense against potential outbreaks, paving the way for a healthier and safer future for all.

by sgn09 | Nov 19, 2023 | Dashboard
HIV persists as a noteworthy communicable disease in Europe and a substantial risk in the Arab world, posing a significant health challenge. This infection is associated with considerable healthcare costs for treatment and care, a noteworthy mortality rate, and a reduction in life expectancy. The virus specifically attacks the immune system, resulting in a persistent and severe illness with an extended incubation period before symptoms manifest.
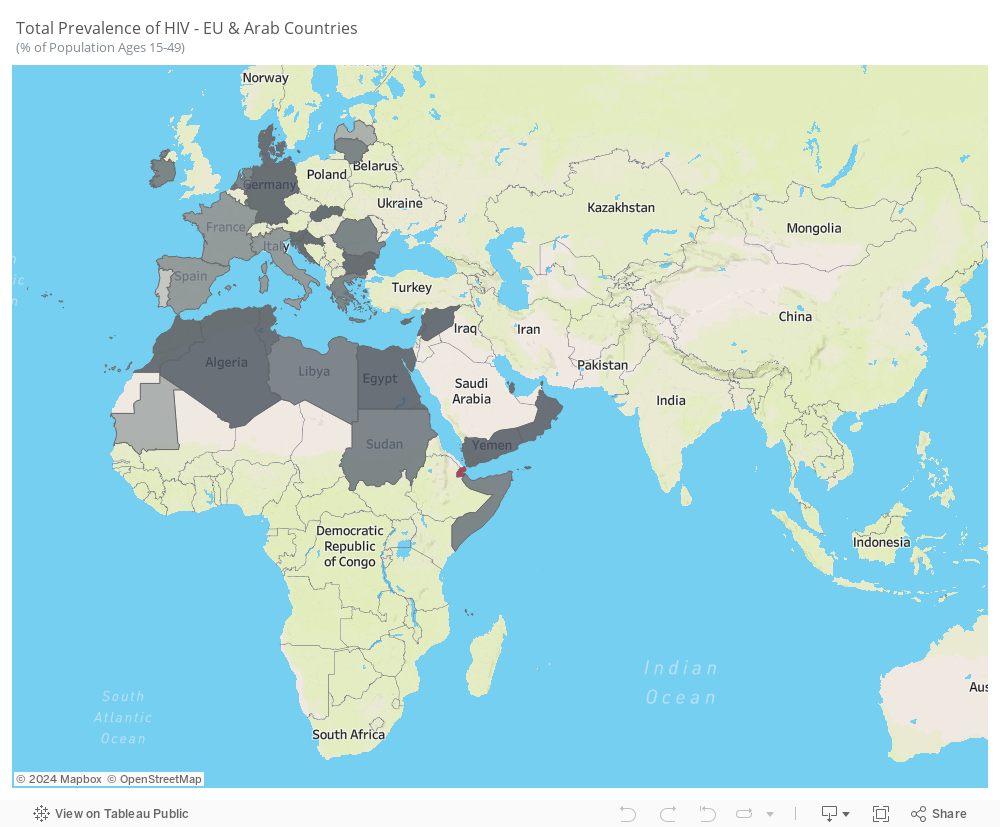
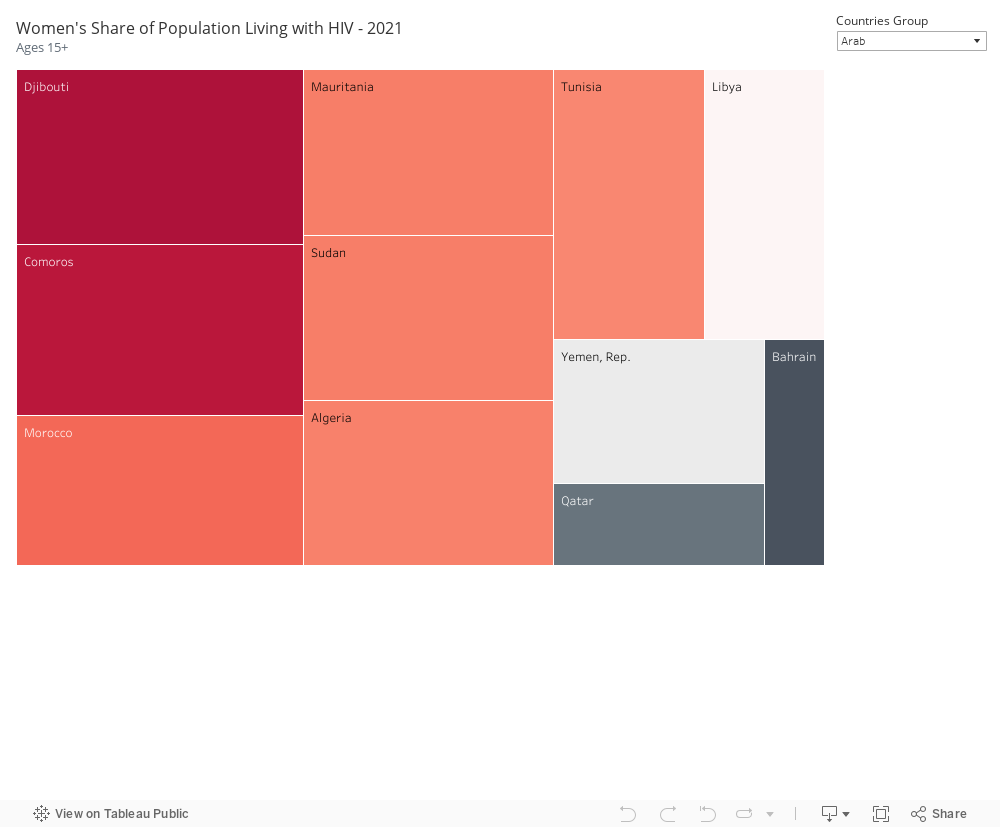
The average prevalence from 2005 to 2021 reveals notable trends. While some Arab countries, like Saudi Arabia, UAE, and Iraq, do not consistently report HIV statistics, the available data highlights the prevalence of the disease in Arab countries situated in Africa. In contrast, European countries, particularly Portugal, Latvia, France, and Italy, exhibit higher prevalence rates.
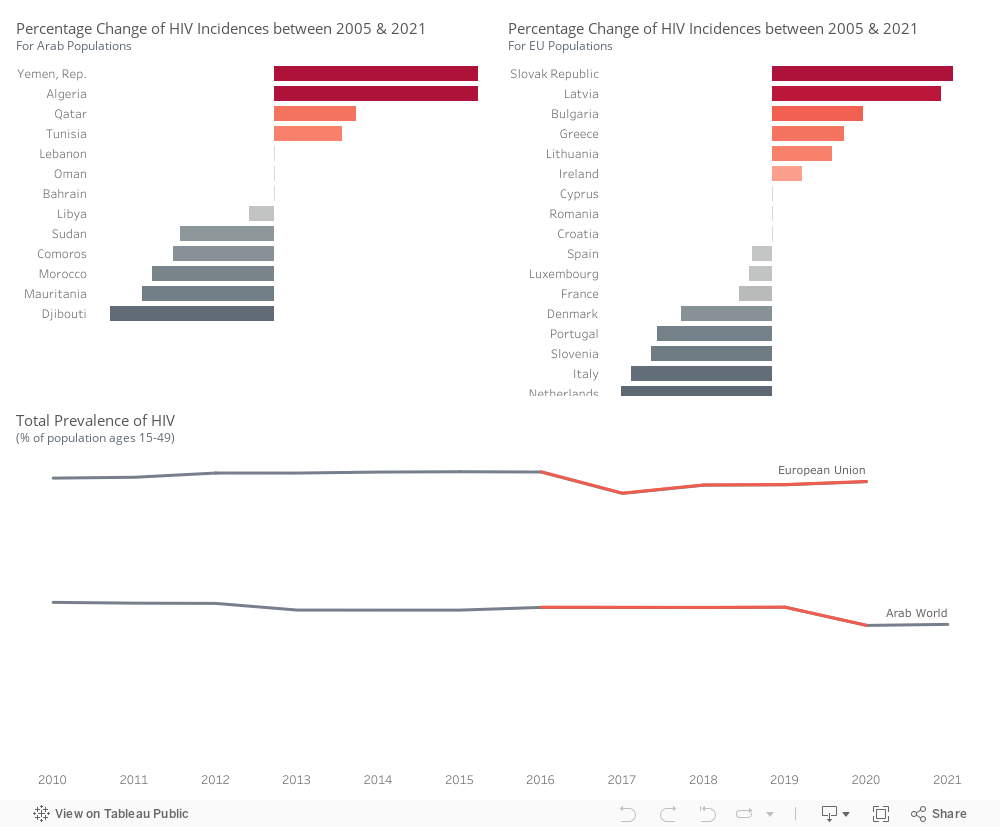
Within the Arab world, there is an upward trend in the percentage of HIV incidences in Yemen, Algeria, Qatar, and Tunisia. Conversely, Djibouti, Mauritania, Morocco, Comoros, Sudan, and Libya exhibit a decline in HIV incidence rates.
Within the Euro area, there is an increase in HIV incidences observed in Slovakia, Latvia, Bulgaria, Greece, Lithuania, and Ireland. However, a decrease is noted in the Netherlands, Italy, Slovenia, Portugal, Denmark, France, Luxembourg, Spain, and Croatia.
HIV prevalence is higher in European Union countries compared to Arab countries. There was an incline in Arab countries around 2020, while in the European Union, the trend experienced a decrease in 2017, followed by a slight upward movement.
We will be focusing on these countries in the following visuals.
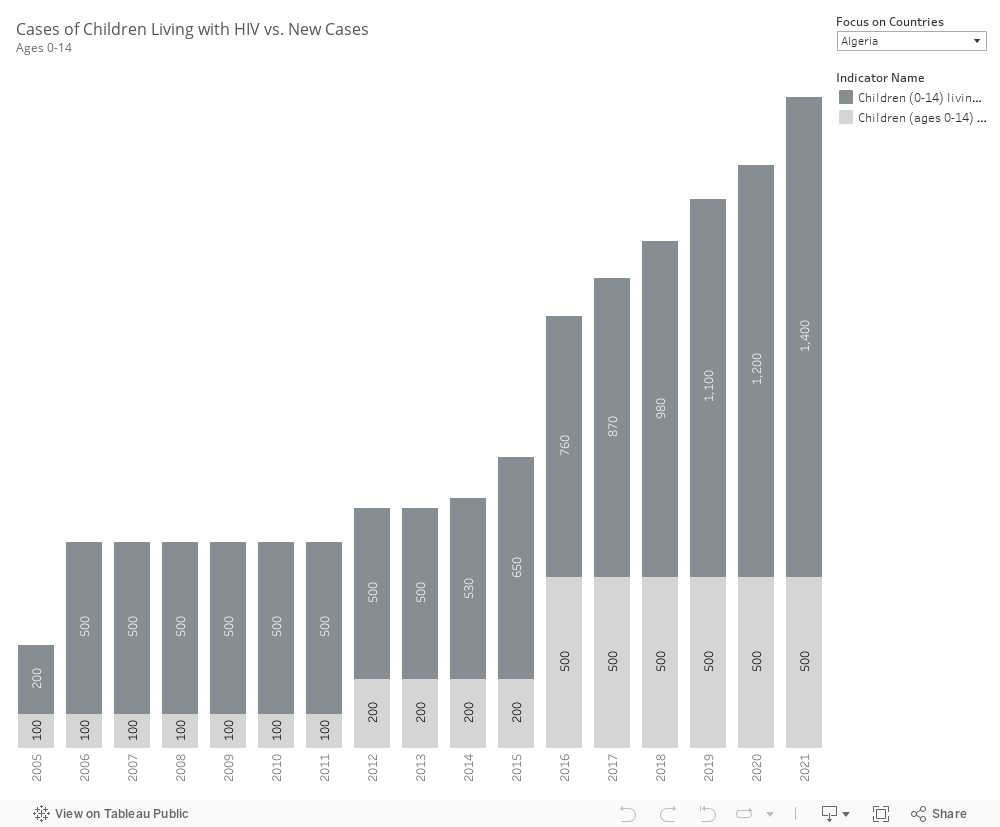
Most countries do not report parameters related to children living with HIV and newly infected children. However, the available data indicates that in Algeria and Morocco, both the number of children infected and the number of new cases are on the rise. In contrast, Djibouti has successfully decreased these numbers, as has Mauritania.
In our selected focus countries, notable instances of HIV infection among the female population are observed. Within Arab countries, Djibouti, Comoros, Mauritania, Sudan, Morocco, Algeria, and Tunisia exhibit a high prevalence. Similarly, in EU countries, France, Portugal, Latvia, Ireland, Luxembourg, and Italy show a high number of females infected with HIV.
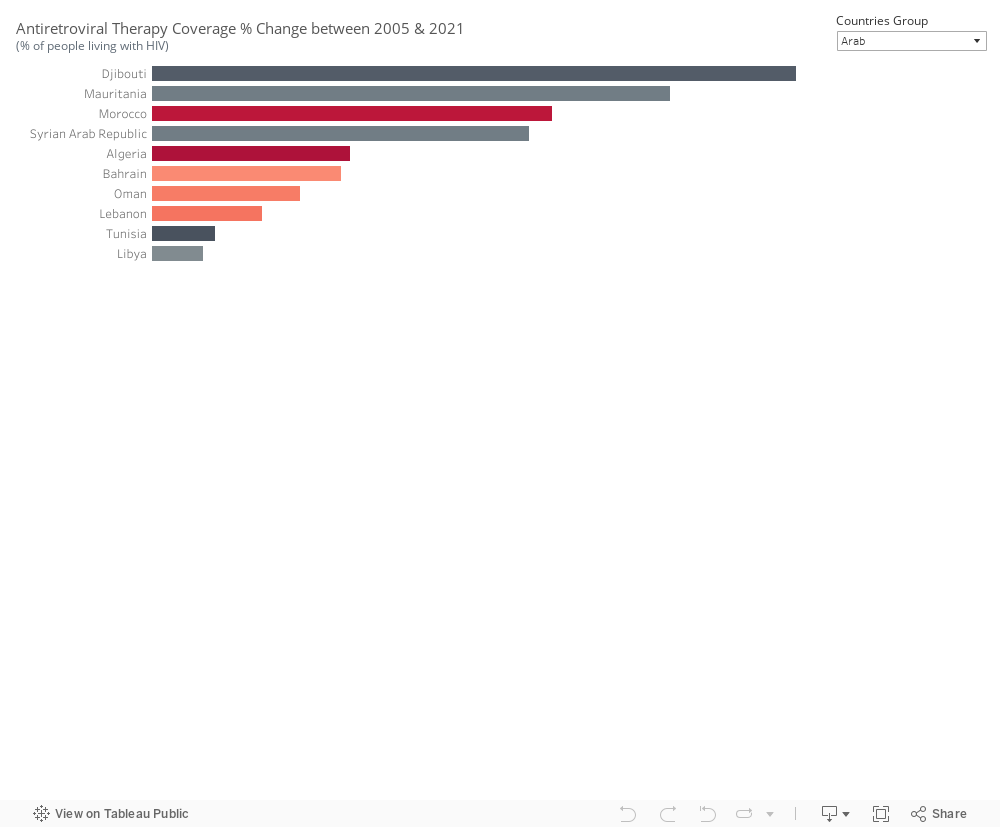
Antiretroviral therapy coverage has seen an increase since 2005 in Djibouti, Mauritania, and Morocco within the Arab world, as well as in Latvia and Bulgaria. The effectiveness of the treatment is reflected in the declining incidence cases observed. However, in Algeria, despite an increase in treatment coverage, the number of incidents continues to rise. A similar situation is noted in Slovenia, suggesting that the treatment alone may not be sufficient to curb the spread of HIV.
Information pertaining to condom use and protected sex is currently unavailable, emphasizing the need to gather this specific dataset.
In conclusion, Europe & the Arab World are far from meeting global HIV targets. Annual new HIV infections from AIDS-related illness are on the rise. While treatment can contribute to reducing the prevalence of HIV in a country, it is just one aspect of a comprehensive approach. Relying solely on treatment is inadequate. Nations should prioritize addressing other impactful factors, including:
- Implementing prevention programs that effectively reach key populations in substantial numbers.
- Making special efforts to enhance and extend HIV testing and treatment initiatives.
- Increasing engagement with the younger demographic.
- Enforcing effective policies such as mandatory testing for work or residence permits, mandatory testing for marriage, and criminalizing activities such as sex work and drug use or possession for personal use.

by iaa28 | Nov 23, 2022 | Uncategorized
Public health is linked to the economic strength of a country as health expenditure is positively associated with the productivity and GDP of a nation. The advances and improvement of many of the main forces driving economic growth over time span such as technological progress, education, and physical capital accumulation contribute to the improvement of health services in countries. However, with the world divided between first, second and third world countries, public health situation differs between economically strong and weak countries.
COVID-19, as a recent event, shed light on the differences in health systems within the Arab world, especially that the region includes some of the richest oil producing countries as well as poor and war-torn countries.
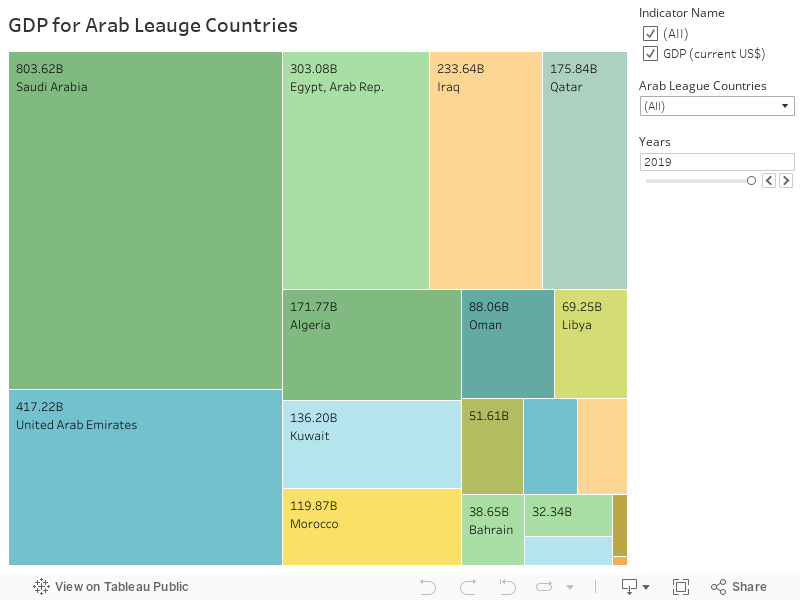
The below graph visually views the differences between the GDP of the Arab League Countries in the Year 2019. For example, at the top of the GDP scale , we have Qatar, a relatively geographically small GCC country and biggest producer of natural gas, has a GDP of $175 billion which is more than GDP of Libya, Lebanon, Sudan and Yemen combined.
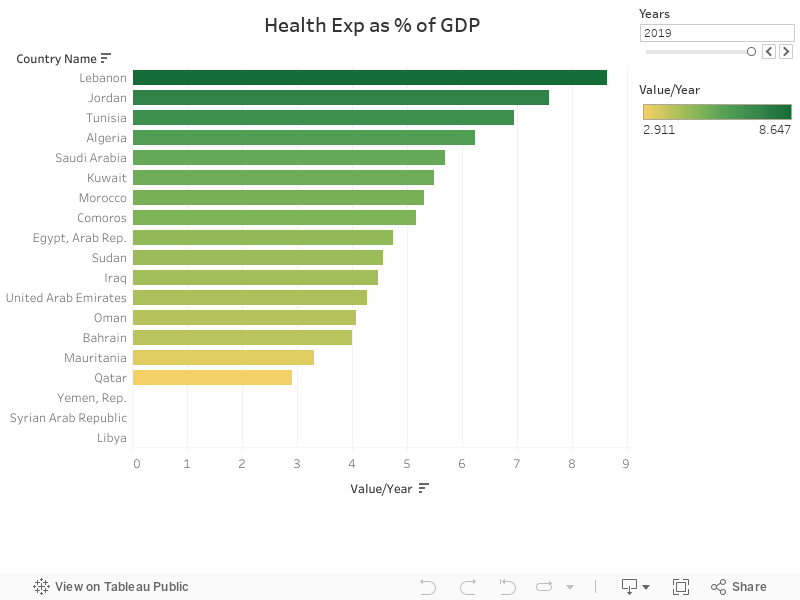
The size of a country’s GDP determines the monetary value of its health expenditure as a percentage of GDP. Comparing the GDP tree map with Health Expenditure graph below , we can see that countries with high GDP (e.g, Qatar, UAE) shows small percentage of health expenditure while Countries with low GDP (e.g, Lebanon, Jordan) shows larger percentage of health expenditure.
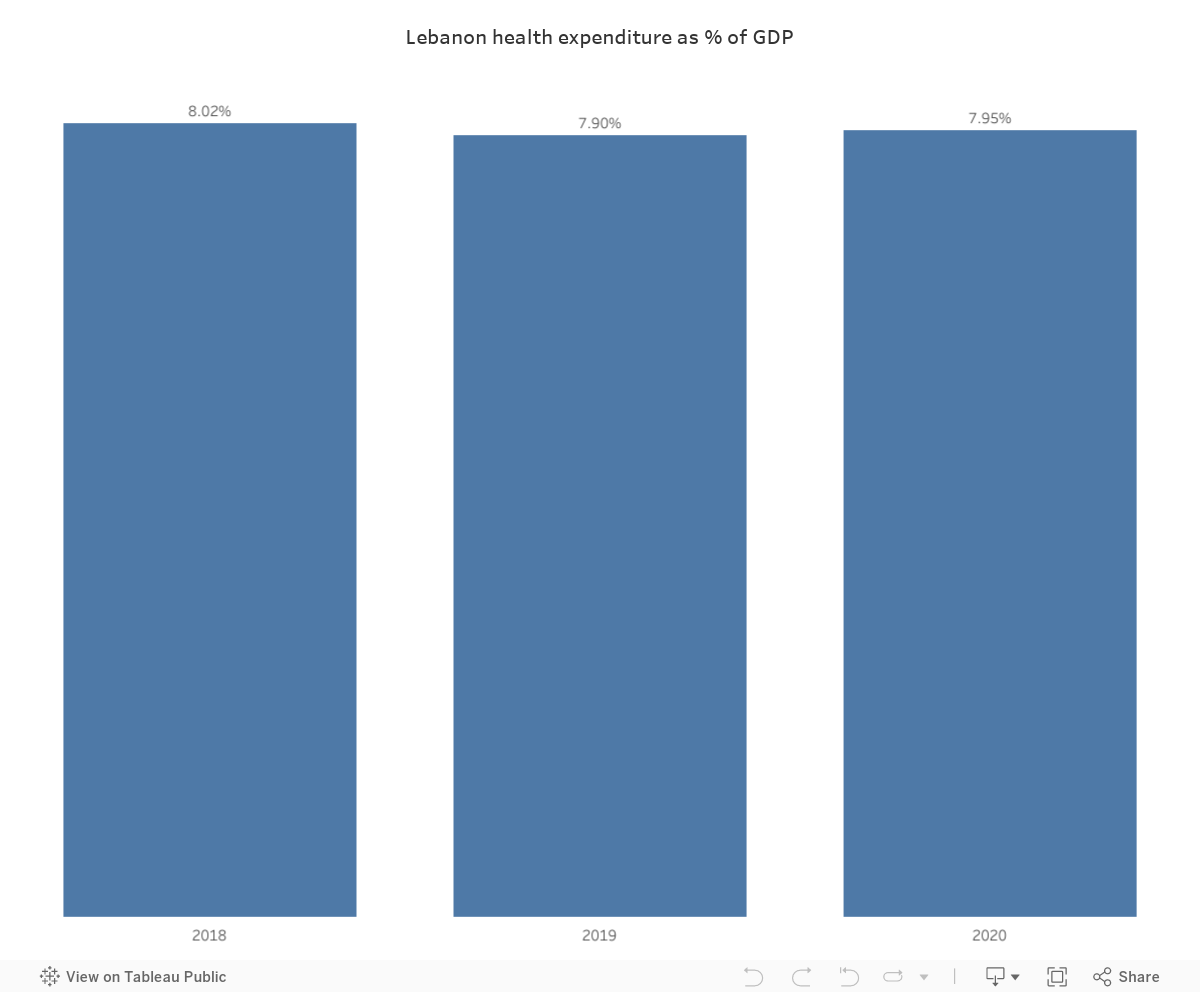
In monetary terms, Lebanon has a highest total health expenditure % in the Arab World which amounts to 8.64%($51.6 B)= $4.45 billion. On the other hand, Qatar has a low health expenditure % of 2.9 but when multiplied by the country’s GDP, it amounts to 2.9%($175 B)= $5 billion.
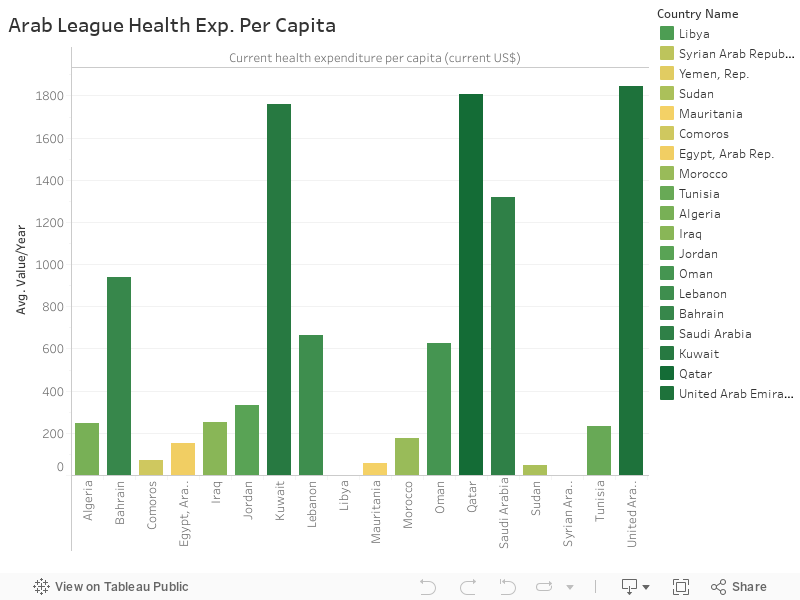
Health Expenditure per capita shows the direct impact of GDP of a country on its health spending. As shown in the below graph, countries with high GDP have high health expenditure compared countries with low GDPs.
The above discussion pointed out the relationship between the strength of a country’s economy and its health spending. The question that remains is “How does this reflect on the health of people?”
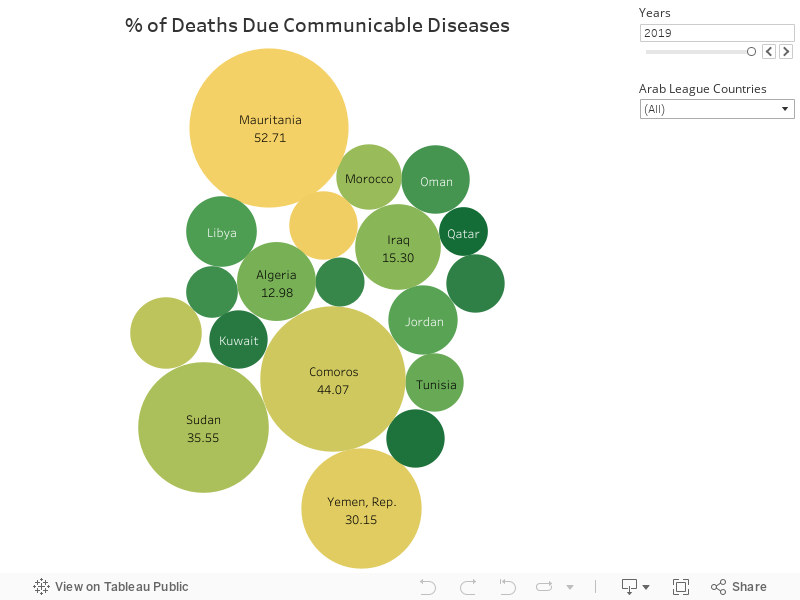
Diseases
Countries that allocate large budgets for the development of the health sector and public health perform well in the face of diseases, especially communicable diseases and pandemics such as COVID-19. The below bubble chart shows that countries with low GDP have the highest percentage of deaths by communicable diseases.
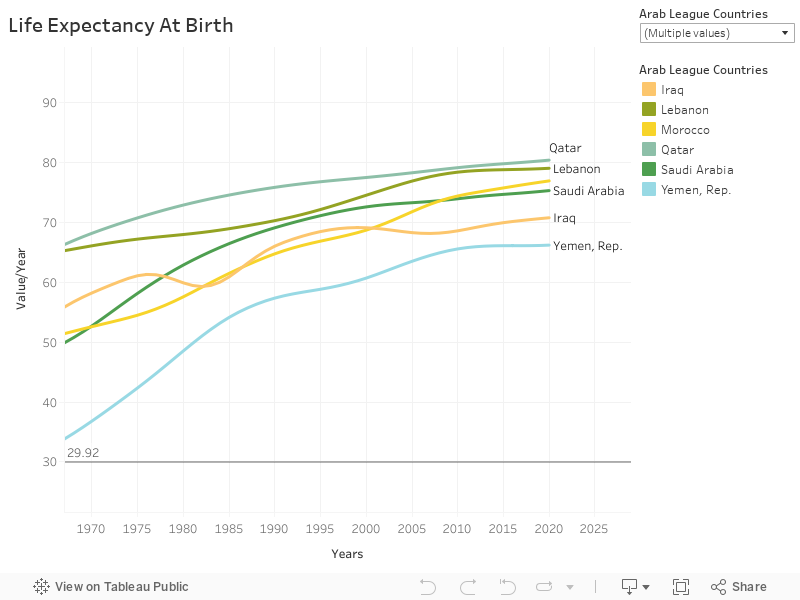
Life Expectancy and Death Rate
To further show the evidence of the impact of GDP and public health spending, we consider both indicators: Life Expectancy at Birth and Death Rate in the Arab League Countries.
- Life Expectancy at Birth: we can that people from countries with high GDPs and high health expenditure per capita. Qatar leads the way with 80 years expected age in 2020 while Yemen has an expected age of 66 years in the same year.
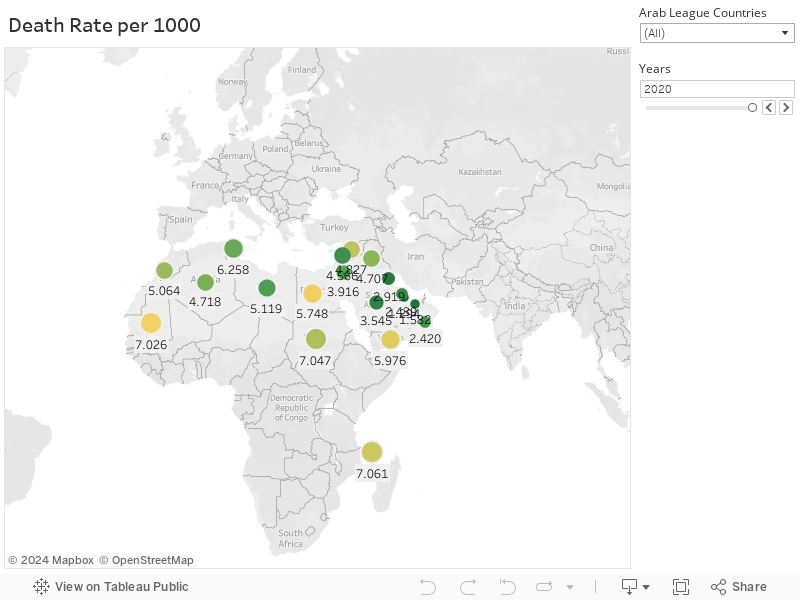
- Death Rate: the same pattern seen with Life Expectancy is also seen in death rates per 1000 persons. Qatar has a death rate of 1.2 compared to Yemen which has a death rate of 5.9, both in 2020.
What should be done?
The United Nations Sustainable Development Goal #3 “Ensure healthy lives and promote well-being for all at all ages” points out the need for improving the public health of the world population. Health spending by governments is a very important factor in the health of their people. However, for those countries who are economically disadvantaged, improving health can be also achieved through:
- Investing in education, especially in medicine studies to make sure the health sector has the competent doctors and specialists.
- Directing international aid more towards developing health sectors in poor countries rather than urgent assistance.
- Investing in awareness: one of the most important ways to improve health in developing countries is by educating citizens to take preventive healthcare measures and avoid riskier health behaviors.