Beyond Bad Luck: Why The Data Shows Rural Lebanon Is a Health Hazard
It was a quiet Sunday afternoon in a small town in the West Bekaa. Two friends, Jad (15) and Rami (14), were enjoying a simple innocent motor bike ride. But unfortunately, they were hit by a speeding SUV.
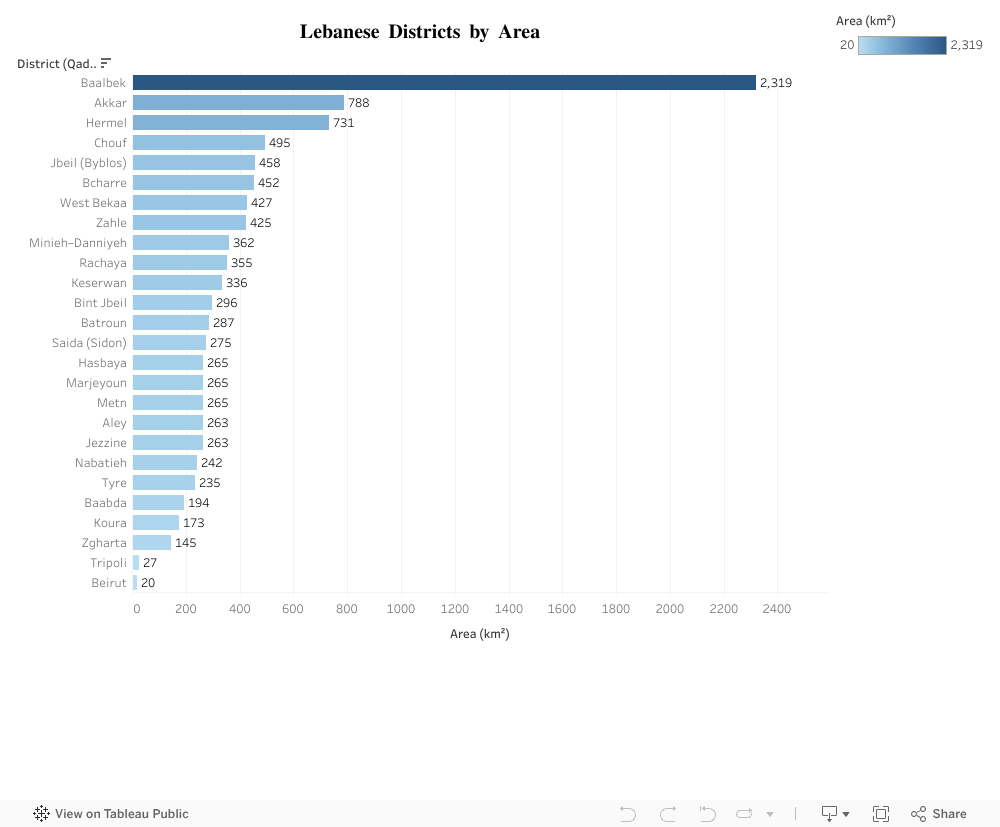
The town folk gathered around the 2 boys that were laying bleeding on the asphalt road. The ambulance arrived quickly. Jad needed immediate, high-level trauma care. He needed a specialized surgeon within minutes. The nearest facility capable of saving his life, however, was in Zahle, a 45-minute drive through challenging rural roads.
For severe trauma, 45 minutes is not a journey, but it is a critical time window that determines fate. While Rami survived after weeks in the ICU, Jad unfortunately bled out on the way.
His death wasn’t solely a result of the collision. But it was a devastating consequence of a systemic, geographical failure.
The Evidence: Mapping the Disparity
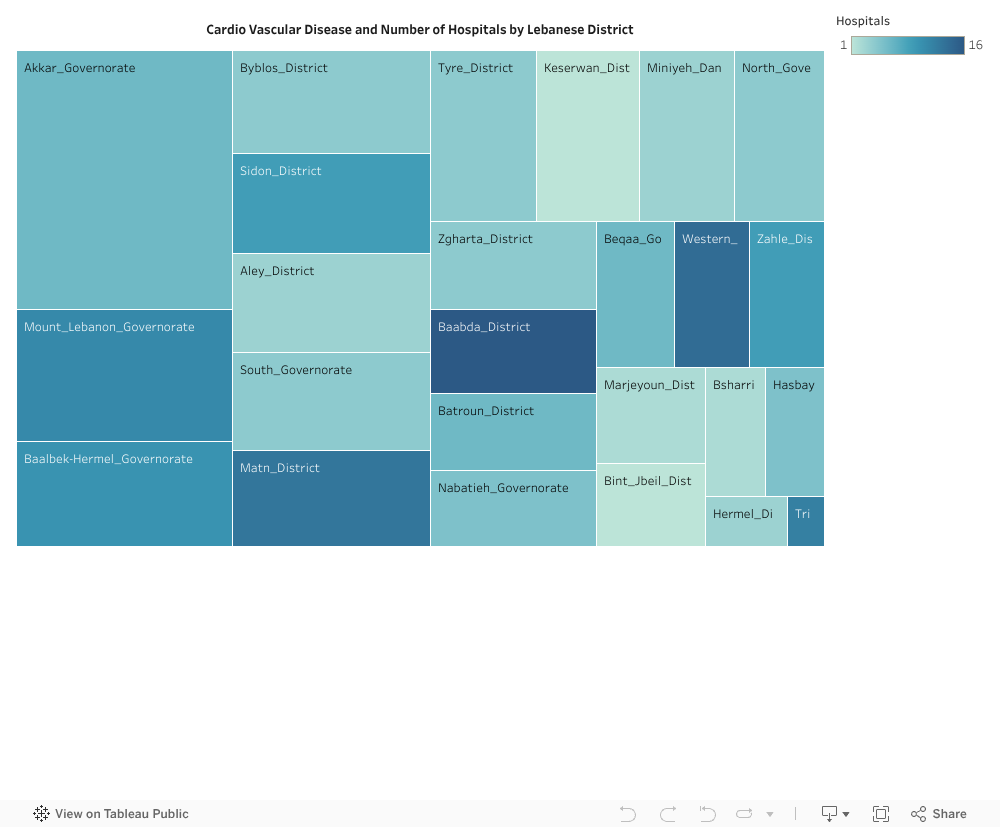
This tragedy is not an isolated incident of bad luck. It is the human cost of a deeply imbalanced healthcare system. Our data analysis confirms what rural families already know: Access to care is dangerously centralized.
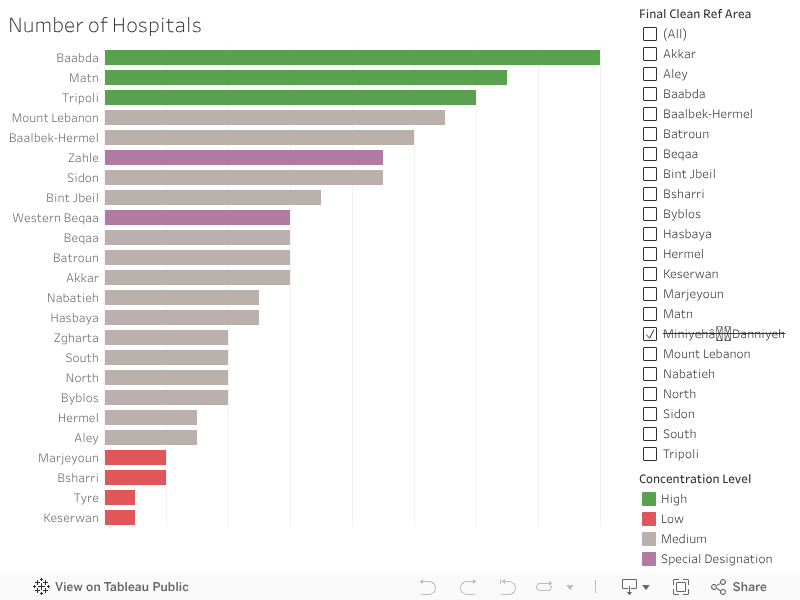
The visualization of medical facilities across Lebanon’s districts illustrates this shocking disparity:
-
The areas highlighted in Green (the top 3) enjoy a dense concentration of hospitals, offering multiple lifelines within minutes.
-
On the opposite end, the areas highlighted in Red (the bottom 4) show bars that are barely visible, confirming these are healthcare deserts.
The system is designed to serve the city, leaving the vast rural expanse with an inadequate margin of error. Your chance of survival is, quite literally, dictated by the proximity of your nearest bar on this chart.
The Solution
We cannot solve the problem of distance by trying to build a new university medical center in every district. That is fiscally impossible. The real solution is smart, targeted investment in stabilizing the patient, not relocating the hospital.
Our data, which shows the alarmingly low density of First Aid and Care Units in the rural areas, points directly to the answer. We must transform these simple clinics into advanced, highly efficient units.

1. Buying Time
The difference between life and death for someone like Jad is the critical time immediately following a severe injury.
The goal of a new, Trauma-Ready Care Unit is to manage and stabilize major injuries (like severe bleeding or airway obstruction) for 30 minutes. It’s not a full operating room, but it has the specialized staff and equipment to:
-
Stop the Clock: Stabilize the patient with basic surgical procedures.
-
Coordinate Transport: Link immediately with air or specialized ground ambulance services.
By creating these small hubs, we effectively shrink the deadly 45-minute travel time into a manageable window, giving the patient the chance to survive the journey to the major hospital.
2. Decompressing the ER
The benefits flow both ways. Today, emergency rooms in major urban hospitals (like those in Zahle or Baabda) are often jammed with non-critical cases:
-
Minor broken bones
-
Deep lacerations needing stitches
-
Dog bites and severe infections
By upgrading rural units, these facilities can handle this high volume of urgent but non-life-threatening cases.
The immediate effect is a massive reduction in pressure on the urban ERs. This allows the major city hospitals to focus their specialized surgeons and resources entirely on the true, severe emergencies, like the trauma case that should have saved Jad.
Big Idea: “Healthcare equality is not just about bringing care closer; it’s about making sure the right care is available at the right time for everyone, everywhere.” Investing in these small, advanced units is the fastest, most cost-effective way to bridge the deadly gap on our map.