by csd04 | Nov 21, 2025 | Generic, Uncategorized, Visualization
In Heart Attacks, Every Minute Lost Reduces Survival
Heart attacks don’t negotiate. Once symptoms start, the countdown begins and survival depends on how fast a patient reaches a hospital that can intervene. This makes geography a health factor.
In Lebanon, where hospitals are not evenly distributed across districts, access time can vary sharply from one place to another. The question isn’t only “how many heart cases do we have?” but also “how close is care when those cases happen?”
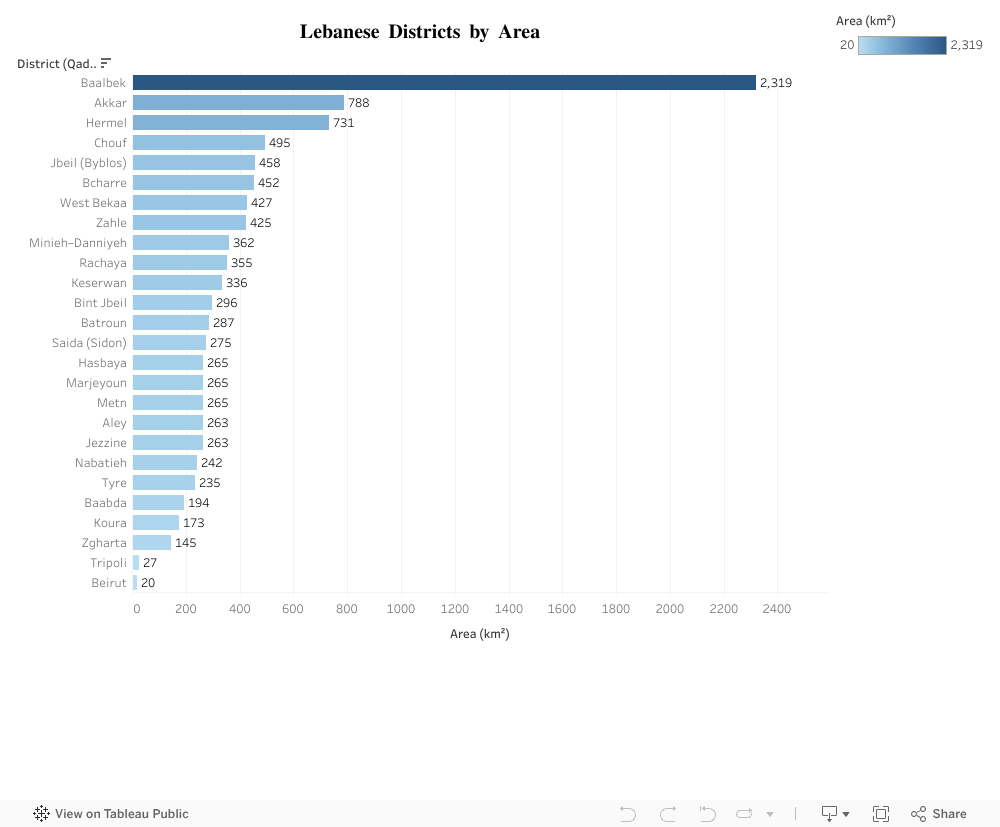
Akkar vs. Baabda: A District Size Contrast That Matters
Akkar and Baabda illustrate Lebanon’s geographic contrasts clearly. Akkar spans 788 km², making it one of the largest districts in the country, with wide and spread out communities. Baabda, by comparison, covers just 194 km² nearly four times smaller.
This difference isn’t just a cartographic detail; it fundamentally shapes residents’ access to services. In a district as large as Akkar, simply reaching a hospital can take significantly more time, while Baabda’s compact size naturally supports quicker, more concentrated access to care.
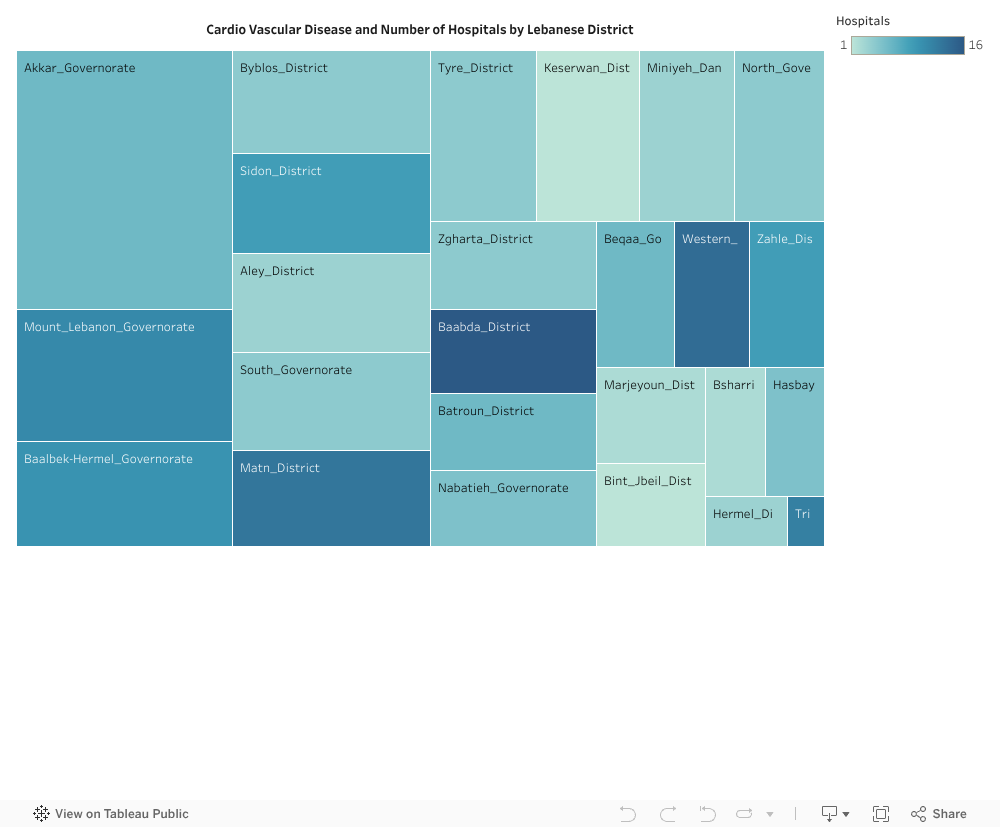
Mismatch between burden and capacity
Akkar also shows a high cardiovascular case load
In other words:
- Big territory → longer distances by default
- Low hospital density → fewer nearby entry points for emergency care
- High cardiovascular cases → more people needing urgent access
That combination is a red flag. It implies that when heart attacks strike in Akkar, residents are more likely to face delayed arrival to care compared to smaller, better served districts.
What could realistically improve this?
This isn’t about building a hospital in every village. It’s about optimizing emergency reach. Lebanon already has health infrastructure, the strategic gap is spatial coverage and speed.
A practical way forward is to reduce time to care in high burden, low coverage districts through targeted interventions such as:
- Upgrading/expanding emergency-capable units in under-served districts
- Deploying advanced ambulance hubs positioned for maximum coverage
- Formalizing rapid transfer pathways to the nearest cardiac-capable hospital
The goal is simple: even if a hospital isn’t next door, the system should behave like it is by cutting delays.
How to prioritize smartly?
The visuals naturally suggest a prioritization logic:
- Identify districts with high cardiovascular cases (large bars / darker heat).
- Among them, flag those with low hospital density (lighter color).
- Cross-check physical area (larger districts imply longer response routes).
Districts like Akkar fall into the high-priority quadrant: large area, high burden, low coverage. These are the districts where a marginal improvement in access time could prevent disproportionately more deaths. That’s high ROI health policy.
Align capacity with need
If we reduce time in districts like Akkar, through more emergency nodes, better equipped local units, or faster transfer networks, we align capacity with need without requiring unrealistic nationwide hospital expansion.
Next Steps?
Lebanon should treat emergency cardiac access as a geographic equity issue. Health planning must go beyond counting hospitals, it should measure how fast people can reach lifesaving care, especially in high burden districts.
Because in a heart attack, there’s no such thing as an average patient. There’s only the patient who needs help now, and whether help is close enough to arrive in time.

by crr08 | Nov 20, 2025 | Uncategorized
Unequal Support: When Small Numbers Hide Real Lives
This is Jane, a 27-year-old Ethiopian domestic worker living in Akkar.
Last month, when she got sick, she had no access to community aid, legal protection, or medical support.
She waited four days before anyone could help her—not because support didn’t exist, but because in Akkar there are too few immigrant workers to be considered a priority.
Jane’s struggle is not personal—it’s structural.
Immigrant workers in Lebanon are not distributed evenly across the country, and when population numbers are small, support systems disappear.
Small communities become invisible, unheard, and unprotected.
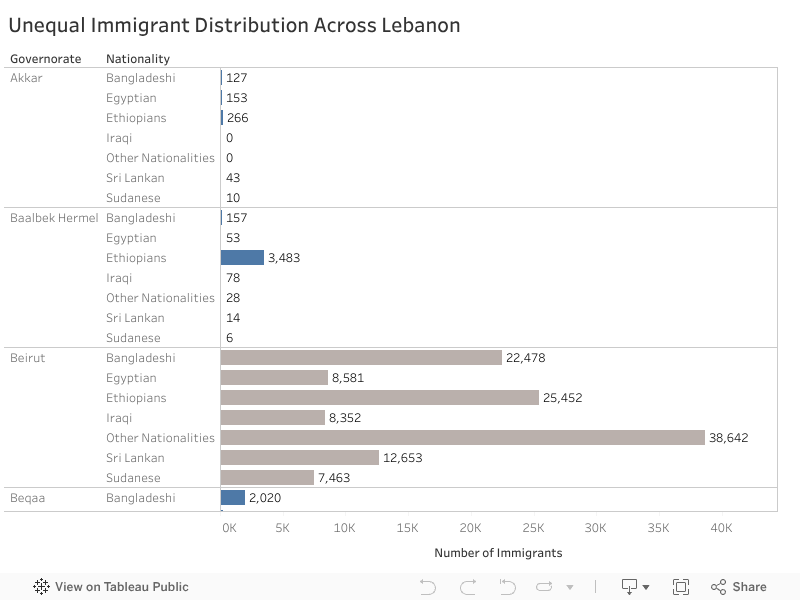
Below is the distribution of immigrant workers across Lebanon by nationality and governorate.
Everything in blue represents a community with fewer than 10,000 workers, meaning low visibility and often no access to essential support.
While Beirut hosts extremely large populations — for example 38,642 workers labeled “Other Nationalities” and 25,452 Ethiopians—governorates like Akkar host only 266 Ethiopians and 127 Bangladeshis.
Yet behind every small number is a real human life.
If We Do Nothing
If nothing changes, workers like Jane will continue to suffer in silence.
Low-population regions will remain overlooked, and inequality will deepen — not because help doesn’t exist, but because help isn’t distributed fairly.
What Can We Do?
Solution 1—Mobile Clinics
Mobile clinics are medical vans that travel to underserved regions to deliver basic healthcare.
They bring support to people who cannot safely or affordably reach Beirut.
During COVID-19, NGOs in Lebanon successfully used mobile medical units to reach remote areas — proving that mobility overcomes geographic inequality.
Solution 2—Rotating Outreach Teams
Teams of legal advisors, translators, and social workers rotate across governorates weekly, providing education, protection, and emergency help.
This approach already works in Jordan, where outreach teams support Syrian refugees in dispersed rural camps without needing permanent offices.
Solution 3—Minimum-Support Policies
A national guarantee ensuring every governorate receives a basic level of support, regardless of population size.
Just as Lebanon provides schools, electricity, and hospitals to small villages, immigrant workers deserve equal dignity and safety.
Findings & Recommendation
Support should not depend on population size — dignity must be universal.
Lebanon should adopt minimum-support policies, expand mobile and rotating services, and ensure that no worker is invisible.
Jane deserves to be seen. Every worker does.

by Sara Dabbous | May 7, 2020 | Dashboard, Visualization
Since I started working in the healthcare sector I’ve always been interested in knowing more about this industry. As such, while exploring the WDI Data I studied several healthcare indicators and it turns out – Lebanon is doing better than we thought! I was intrigued to know what’s beyond those indicators, and luckily I found a detailed dataset about Primary Health Care Centers in Lebanon on The Humanitarian Data Exchange, I was surprised to know we had this many centers.
Could this visualization be a sign of a sound healthcare system ?
Did this awareness in healthcare aid us in containing the Covid-19?
Do you think there is a better future for the healthcare system for Lebanon, or will it be worst?
Personally, I am optimistic..
So here are some things I didn’t know:
- There are 174 Operational Primary Healthcare Centers in Lebanon
- There are 25 PHC funded by UNHCR
- There are 100 PHC that provide subsidized services.
- Nabatieh has 0 operational PHCs.
- The North governorate has the highest number of operational PHC: 36

In this dashboard, I prepared – using Tableau – a map that shows the different Operational PHC locations in Lebanon filtered by UNHCR Funding. Alongside it, is a bar chart showing the percentage of operational PHC in each Governorate. Finally, at the bottom, you can find a stacked bar chart representing the number of operational PHC per governorate, highlighting those who offer subsidized services.