During the peak of the COVID-19 pandemic back in 2021, waking up to news of people passing away due to symptoms complications became the norm, but in the midst of the overwhelming news, one man’s story hit us hard. His name was Nader, a 46-year-old from Baabda, a man known for his loud laugh, strong coffee, and long Friday lunches with friends. We knew him as the “office guy”; he was in fact there for everyone, until the day when his lungs failed him. He caught COVID, the symptoms escalated quickly. Within days, his oxygen levels dropped, and despite being admitted to the hospital, the virus was already overpowering a weak cardiovascular system. Everyone was in shock, since Nader was just in his mid-40s, and we expected he’d beat the virus easily. But once the doctors informed us he didn’t make due to his overworked cardiovascular system, we understood it was beyond COVID-19, and not only Nader’s lungs have failed him, but a whole lifestyle and healthcare system.
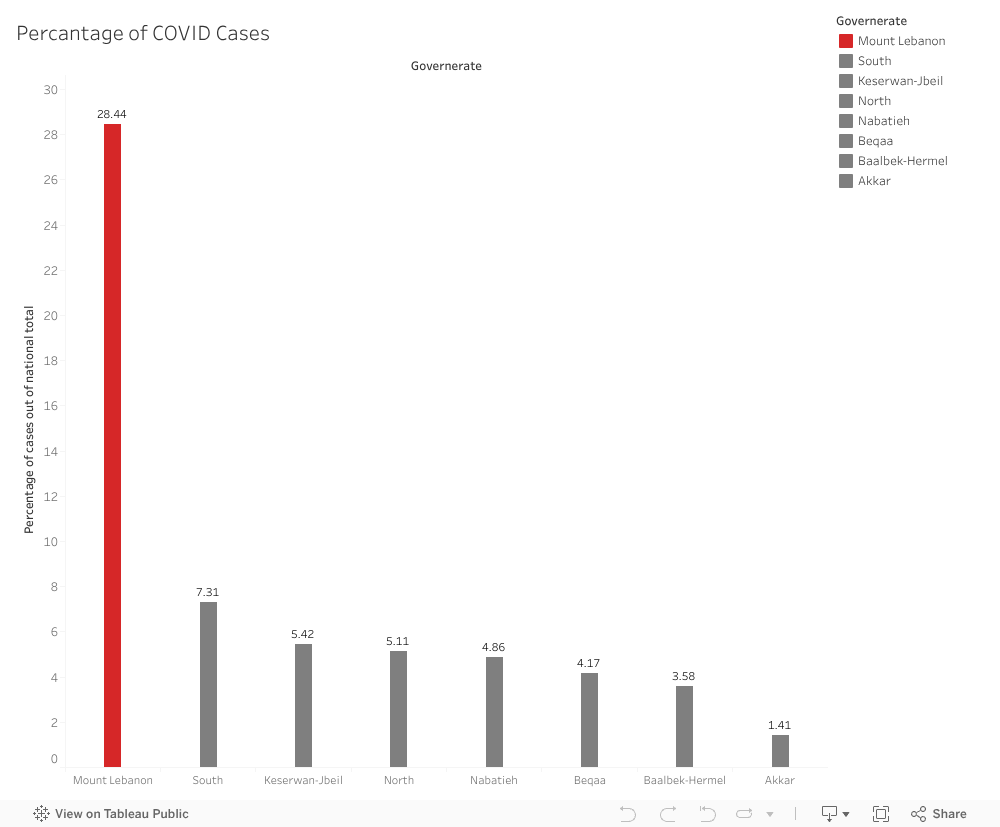
This raised a bigger question for us: Which areas in Lebanon have unusually high levels of chronic disease that make its residents more at risk during crises? To explore this, we analyzed health data across governorates, focusing on cardiovascular disease (CVD) and hypertension (HTN). We first explored how the percentage of COVID-19 cases out of national totals was distributed, with Mount Lebanon leading in this area.
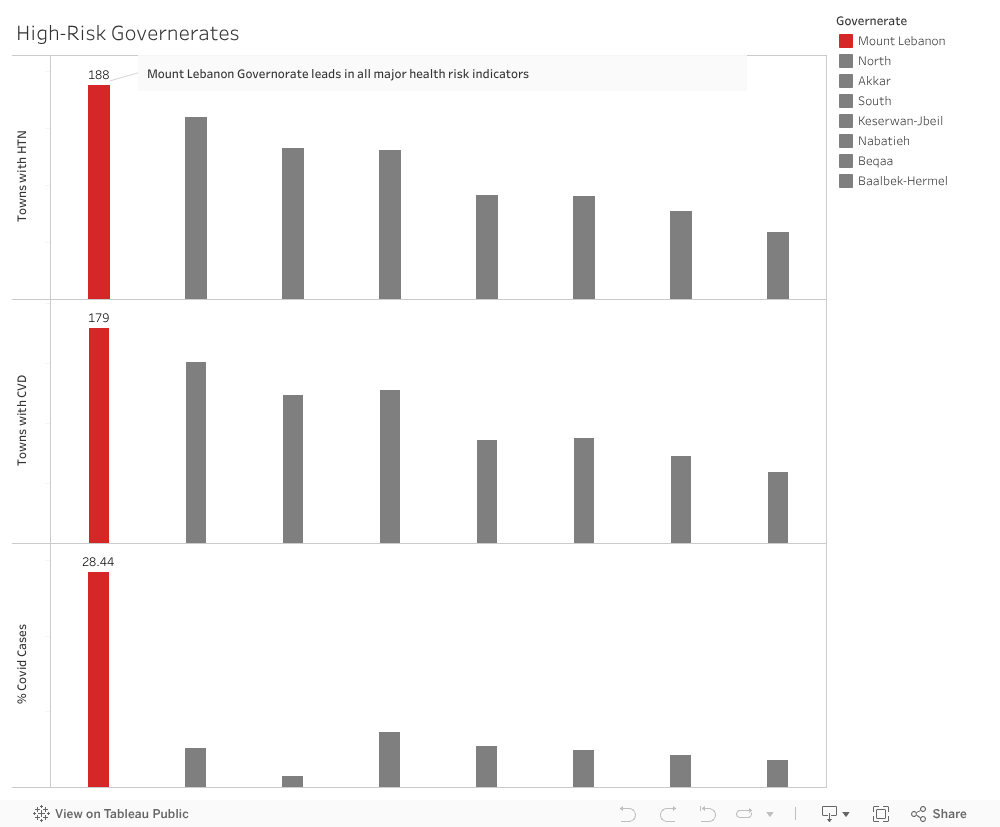
To understand further the extent of the health risk, we compared these chronic disease patterns to COVID cases in all Lebanese Governorates. What we saw flagged Mount Lebanon as a hight risk Governorate as it has the regions with the highest burden of CVD and HTN also recorded the highest COVID cases. This means that in these areas, the symptoms of COVID-19 will be exacerbated by the existing chronic disease, which leads to more complicates and higher hospitalization rates.
The highest-risk governorate being Mount Lebanon isn’t only about pandemic response. It’s about addressing the silent epidemic of chronic disease that makes future health crises even more dangerous. Based on our analysis, we believe it’s time to expand early screening programs, increase community-level hypertension detection, and strengthen preventive care. Preventative measures are needed so that the most vulnerable groups are able to cope with unprecedented health emergencies. If we focus on prevention now, we can reduce risk and help ensure that stories like Nader’s don’t repeat themselves.
This does not start with a funny caption or a happy anecdote, but I assure you it’s an important topic and it touches the lives of everyone. This is Tarek Moukalled, and I hope that by the end of this session you can see the light at the end of the tunnel for patients in Lebanon.
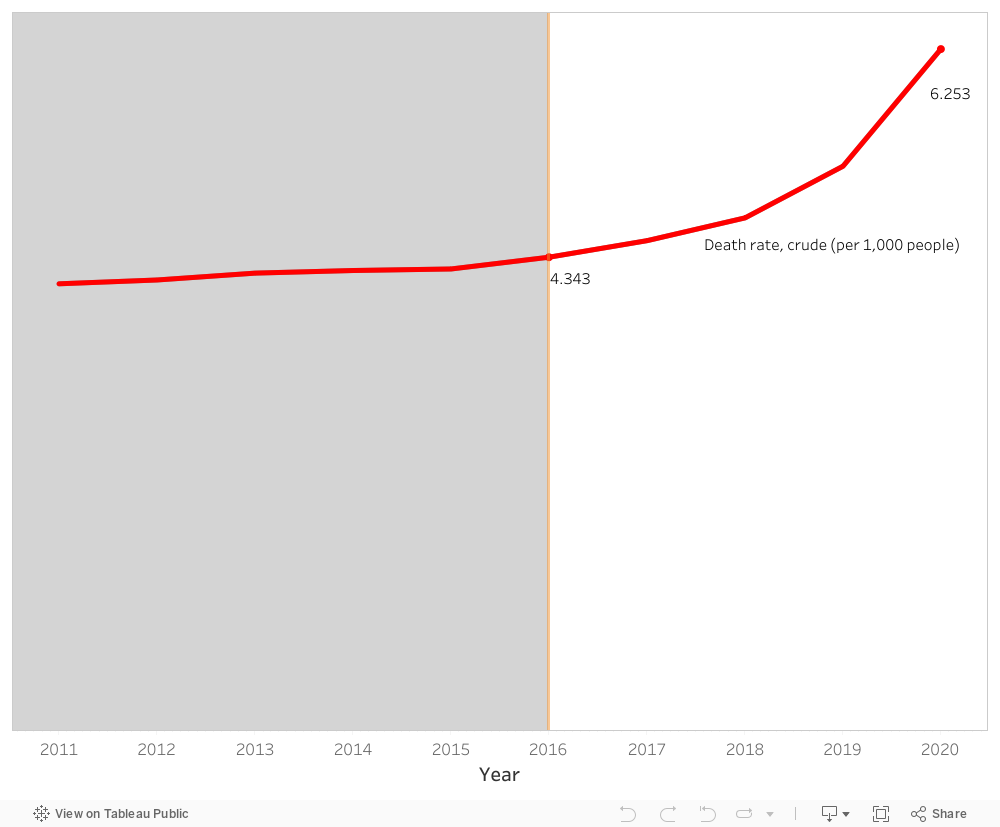
Our story begins with rather an unfortunate observation. Patients in Lebanon are dying. As a matter of fact, the death rate has increased from 4.34 deaths in 2016 to 6.25 deaths in 2020 per 1,000 persons. That is drastic and an alarming increase of approximately 44 % during a span of 5 years. But why?
A close inspection of the healthcare expenditure per capita during the suggested years shows a considerable increase from 648 USD to 995 USD. Furthermore, the % expenditure of GDP on healthcare in Lebanon also shows a consistent trend of a little less than 8 % across the same years. So, things should be fine, if not better! Yet unfortunately, this is not the case.
It appears the Lebanese people have been taking things into their hands. With the economic recession and the subsequent governmental bankruptcy, GDP decreased from ~ 51.1 billion USD in 2016 to 31.7 billion USD in 2020. This led to the fact that the Lebanese people have been paying more and more from their own pockets for healthcare reaching a whopping 44.2 % of healthcare expenditure in 2020.
Comparing the above results with the healthcare sector of a different country that shares similar demographics and healthcare expenditure with Lebanon would help with the context and the subsequent validation of the proposed solution, the light at the end of the tunnel. Remember?
With a similar % expenditure of GDP on healthcare (~ 7.5 %) and a little lower starting point in death rate of 3.16 per 1,000 persons, Jordan’s death rate in 2020 reaches 3.47 per 1,000 persons. The healthcare expenditure per capita in Jordan is consistently way lower than that of Lebanon. The % of out-of-pocket expenditure on healthcare is also steady and lower than that of Lebanon. As to the GDP, it starts lower than Lebanon in 2016 at ~ 39.9 billion USD and ends higher than Lebanon at 43.6 billion USD. As such, the main considerable deviation between both countries is the GDP amount. For that matter, it’s important to note that economies and healthcare sectors grow through expenditure rather than stagnation or restriction.
The increase in the share of health expenditure as part of GDP will have positive results on both short-term and long-term.
Enhanced Healthcare Quality
Faster Healthcare Response
Improved Patient Health Outcome
Decreased Death Rate
Target for Healthcare Tourism
With that, it is imperative to urge whoever who is responsible to proceed with the increase in healthcare expenditure for the sake of our patients and our future.
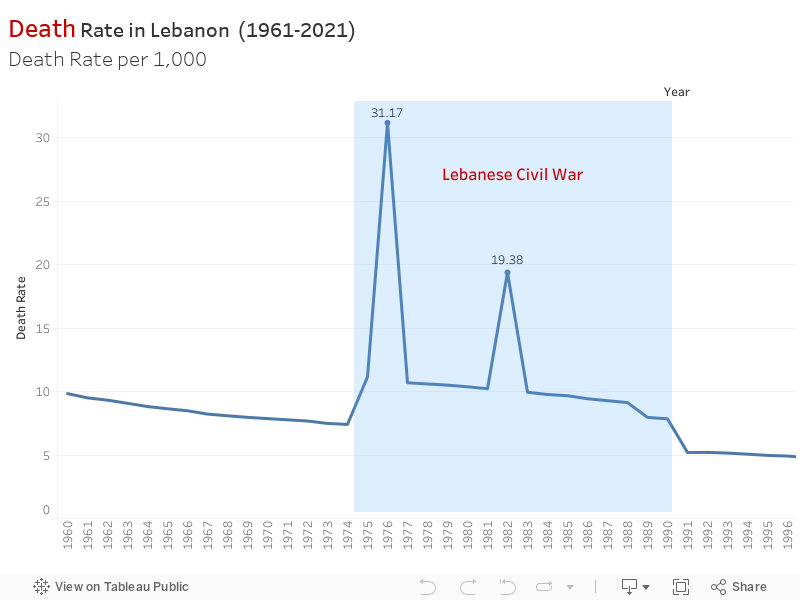
In light of recent events, we delved into a pressing issue: the unsettling fluctuations in mortality rates in Lebanon. It was evident that these shifts had deeper roots, impacting lives and reflecting significant historical events.
The data painted a stark picture. Between 1975 and 1990, Lebanon witnessed a devastating surge in mortality rates, reaching a staggering 31.17. The Lebanese Civil War cast a long shadow, leaving behind a legacy of loss and devastation that echoed in the mortality records.
Post-1990, there was a semblance of stability with mortality rates hovering around 4-5, despite intermittent spikes like the one in 2006 during the July War. It seemed like a fragile peace amid lingering echoes of conflict.
Then, at the dawn of 2019, another dramatic shift occurred. The onset of the COVID-19 pandemic jolted mortality rates sharply upward once more. It was a distressing reminder of how swiftly external factors could disrupt the delicate balance of life.
Contribution to SDG
SDG 3: Good Health and Well-being: The significant increase in mortality rates during the Lebanese Civil War, subsequent fluctuations due to regional conflicts like the July 2006 war, and the sharp increase attributed to the COVID-19 pandemic highlight the importance of SDG 3. It emphasizes the need for resilient healthcare systems, disease prevention, and access to quality healthcare, especially during periods of conflict and health crises.
SDG 16: Peace, Justice, and Strong Institutions: The impact of the Lebanese Civil War and regional conflicts on mortality rates underscores the relevance of SDG 16. Ensuring peace, stability, and strong institutions is vital to prevent the adverse effects of conflicts on public health and to establish systems capable of effectively managing crises and their aftermath.
SDG 10: Reduced Inequalities: The fluctuations in mortality rates due to historical conflicts and the COVID-19 pandemic might reveal disparities and inequalities in healthcare access, response, and resilience. Addressing SDG 10 involves reducing these disparities, ensuring equitable access to healthcare services, and mitigating the disproportionate impacts of crises on vulnerable populations.