by mfe22 | Nov 22, 2025 | Visualization
You inhale 22,000 breaths a day. How clean are they?
Air pollution is invisible, yet it is one of the most harmful elements we are exposed to every day. A major contributor to this pollution is PM2.5 — fine particulate matter that measures 2.5 micrometres or smaller. These particles are small enough to reach deep into the lungs and enter the bloodstream, posing serious risks to heart and respiratory health. PM2.5 levels are measured in micrograms per cubic metre (µg/m³), the global standard for assessing air quality.
In this analysis, I explored how Lebanon compares to its neighbouring countries and to global regions from 2009 to 2019. The findings tell a decade-long story of stagnation and persistent pollution.
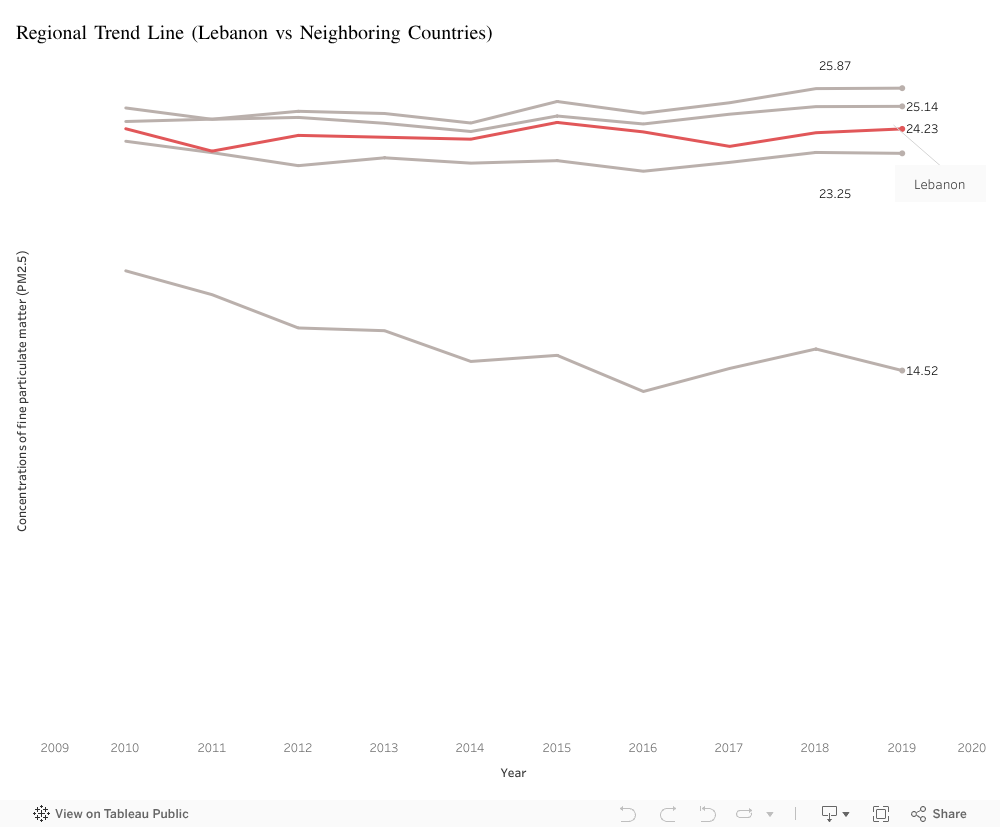
Lebanon vs its Neighbors: A Decade of Stagnation
Over the past decade, Lebanon’s PM2.5 concentration has fluctuated between 23 and 25 µg/m³. While these values place Lebanon below Syria and Turkey, they remain significantly above Cyprus, which consistently records some of the cleanest air in the region. Jordan, though varying slightly year to year, also remains well above safe limits.
Despite these differences, all five countries share one concerning trend: no noticeable improvement over ten years. Lebanon’s air has remained essentially unchanged, offering no signs of meaningful progress in pollution reduction.
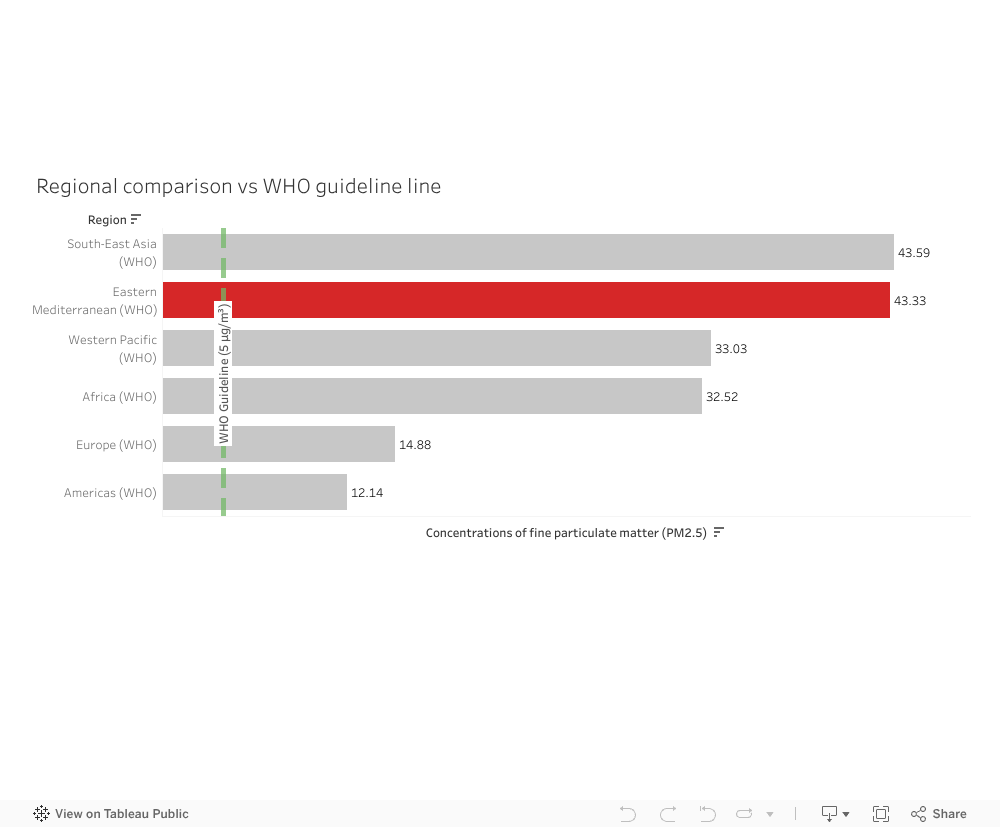
How the Middle East Compares to the World
When placing Lebanon’s situation into a broader context, a clearer imbalance emerges. The Eastern Mediterranean region, which includes Lebanon, records an average PM2.5 concentration of 43.33 µg/m³—almost nine times higher than the WHO annual guideline of 5 µg/m³. Only South-East Asia performs slightly worse.
Regions such as Europe and the Americas fall between 12 and 15 µg/m³, much closer to safer exposure levels. This highlights a stark contrast: the Middle East is one of the most polluted regions in the world, and Lebanon sits within this larger environmental challenge.
Why This Matters
A decade with no improvement in air quality means long-term exposure to harmful particles. PM2.5 is linked to respiratory diseases, cardiovascular complications, and reduced life expectancy. Lebanon’s stagnant pollution levels—paired with its region’s exceptionally high averages—underline the need for stronger environmental policies, emission control strategies, and long-term monitoring.
Conclusion
You inhale 22,000 breaths every day. If the data tells us anything, it is that the air behind those breaths is far from clean. Lebanon’s pollution levels remain elevated, unchanged, and embedded within a regional landscape that struggles with some of the highest PM2.5 levels globally. Understanding these patterns is a first step toward addressing them.

by zct01 | Nov 21, 2025 | Uncategorized
A Morning in Akkar
Somewhere in the hills of Akkar, a mother wakes before dawn. Her son is burning with fever, his tiny chest rising in short, frightened breaths.
She wraps him in a blanket, steps outside and faces the same impossible truth every family in her town lives with:
There is no clinic here.
No doctor.
No nearby care.
The closest medical help is more than an hour away—if roads are clear, if transportation can be found, if nothing goes wrong. For her, and for nearly half of Lebanon’s towns, simple illnesses can become life-threatening journeys. It is not just a healthcare issue, It is a daily, silent tragedy that shapes entire lives.
What the Data Shows but the Country Ignores
The visuals map this tragedy with painful clarity.
In the bar chart:
-
49.74% of Lebanese towns have no local resources nor nearby healthcare.
-
17.08% have no local facilities but can sometimes reach distant care.
Only 33.19% enjoy the basic dignity of accessible treatment.
The map shows Lebanon carved into colors that reveal the geography of abandonment.
-
Akkar, North Lebanon, Baalbek-Hermel, and Bekaa glow in urgent shades of red.
-
Beirut and Mount Lebanon rest confidently in green.
-
Though South Lebanon contains the highest danger percentage, it is covered with governorates that contain abundant amount of medical facilities and resources.
The visuals prove what families in rural regions already know: healthcare access in Lebanon is not just unequal—it is deeply, structurally unfair.
The danger zones are not random, they follow the borders of poverty, neglect, and distance.
A Country at a Crossroads
Yet Lebanon is not without hope. Around the world—and even within its own borders—innovative models show that remote and underserved communities can receive consistent care. The country stands at a crossroads where solutions are known, feasible, and within reach.
Lebanon can choose a future where no mother must gamble with her child’s life because of distance.
That future begins with a hybrid healthcare access model designed for real Lebanese terrain, real Lebanese families, and real Lebanese limitations.
Building the Path Forward
The path unfolds in two phases—immediate relief and lasting transformation.
Immediate Relief
-
Mobile clinics traveling weekly into remote towns.
-
Telehealth services connecting residents with doctors online.
-
Community health workers offering first aid, monitoring chronic diseases, and stabilizing emergencies.
These solutions bring healthcare to the people, rather than asking the people to chase it.
Long-Term Transformation
-
Expanding rural Primary Healthcare Centers (PHCs) in governorates painted red in the danger map.
-
Incentivizing private and nonprofit partnerships to open satellite clinics.
-
Improving transportation links so that even without a local clinic, emergency care is reachable.
This approach does not just fill gaps, it builds a system where every town becomes medically reachable, no matter how far, no matter how rural.
Why This Will Work
Proof already exists.
Organizations like MSF, the Lebanese Red Cross, and multiple NGOs have successfully delivered mobile and remote care across Lebanon’s hardest-to-reach regions. Telehealth has grown worldwide, saving millions in rural communities and the data that drives these charts, maps, and analyses pinpoint exactly where interventions must be prioritized.
The strategy aligns with Lebanon’s national health vision and mirrors international best practices in countries with similar geography and instability.
It is not theory.
It is tested, validated, and realistic.
Beyond the Diagnosis
The visuals do not simply highlight shortages, they illuminate where change must begin.
The Truth
-
Lebanon’s healthcare inequality is regional and predictable, not accidental.
-
Rural northern and eastern regions are in critical danger, lacking both local and nearby care.
-
Nearly half of Lebanese towns face severe accessibility barriers.
The Solution
-
Deploy mobile and telehealth clinics immediately to stabilize high-danger governorates.
-
Invest in long-term PHC expansion to ensure durable access.
-
Integrate transportation and healthcare planning, recognizing that distance is often deadlier than disease.
-
Maintain data-driven monitoring to continuously reallocate resources to evolving needs.
If Lebanon acts now and not later, the red zones can fade. Families can breathe easier. Lives can be saved.
A Different Dawn
One day, perhaps, a child in Akkar will still wake before dawn—but instead of gasping for breath, he will leap from bed to greet a new school day. His mother will no longer fear the distance to care.
Because care will finally be within reach. Because the map will no longer define who survives and who struggles. Because Lebanon will have remembered its forgotten towns.
That is the story the data tells. That is the story this country can still rewrite.
“We are alive the most when we are faced with adversity like no other.”

by jta20 | Nov 21, 2025 | Visualization
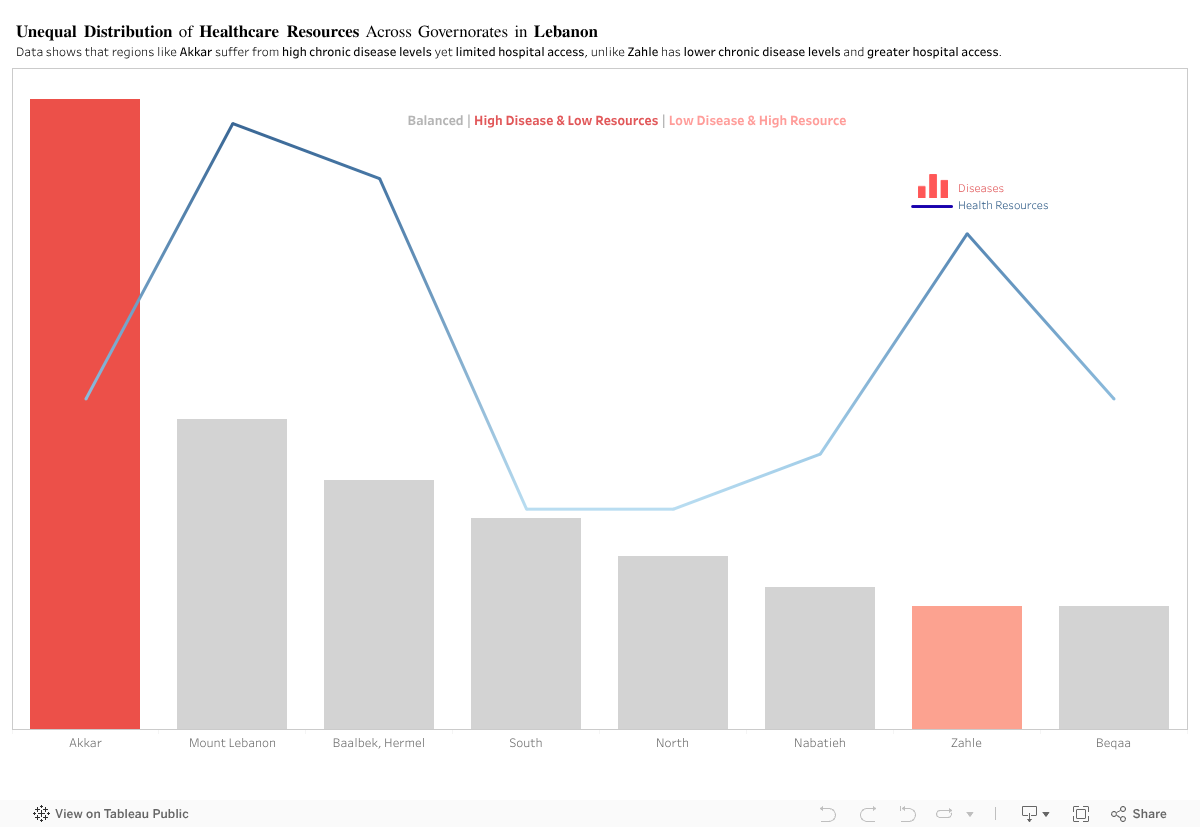
In principle, regions with higher disease levels should have stronger access to healthcare resources. This visualization, however, shows a different pattern.
For this analysis, I compared two indicators across Lebanon’s Governorates:
(1) Diseases
(2) Access to Health Resources
Akkar: High Disease, Limited Access
Akkar consistently shows some of the highest chronic disease levels, yet it has one of the lowest levels of hospital access among the regions.
Zahle: Lower Disease, Higher Access
In contrast, Zahle displays lower disease levels but relatively higher access to hospitals.
By comparing disease levels with healthcare access, the visualization shows a clear mismatch across several governorates. Akkar and Zahle represent two opposite cases, yet the overall pattern remains consistent: health needs and available resources are not aligned across Lebanon.
This raises a key policy question: Are healthcare resources being allocated based on current population needs, or on outdated infrastructure patterns? The evidence suggests that capacity does not scale with actual disease burden in several regions.
To address this, the government should:
- Conduct a nationwide needs-based healthcare assessment to map disease burden against current facility distribution.
- Reallocate resources and funding toward governorates with persistent gaps, particularly in high-need, low-access areas like Akkar.
- Implement dynamic resource planning models that adjust allocations annually based on updated health data.
- Expand primary healthcare centers in underserved regions to reduce pressure on major hospitals.
- Improve transportation and referral systems to ensure patients in remote areas can reach care efficiently
This isn’t about hospital numbers. It’s about a system that gives some regions a chance and leaves others without one.

by rah122 | Nov 20, 2025 | Uncategorized
It is 2015, Samer (13-year-old), just got from school with a strong fever, headache, and tiredness but what was different is the swelling around his jaw area. His parents took him to the doctor and he was diagnosed with Mumps.
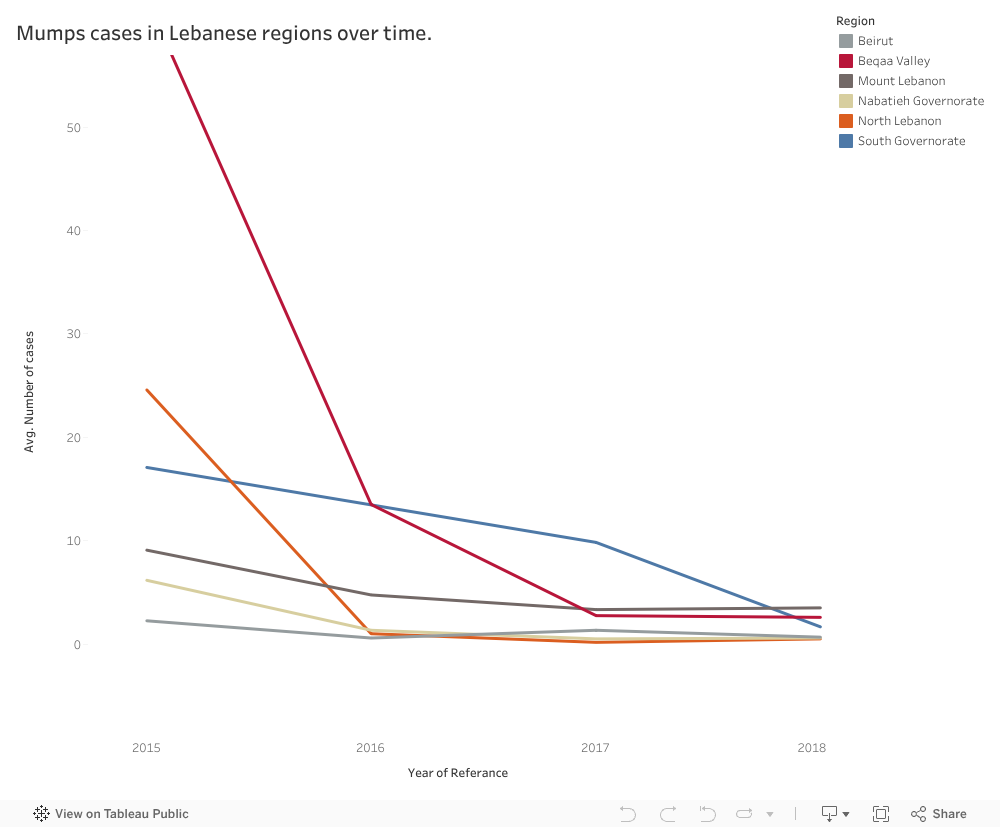
Days later, the school notified all parents of an outbreak in Mumps among students. And what was a school-level problem turned out to be a result of a nation-wide outbreak.
This line graph shows how the number of recorded Mumps cases in 2015 was higher than the years that followed, and this was caused primarily by outbreaks in certain governorates. For example, in 2015 each town in Beqaa valley recorded 62.5 Mumps cases over the year, another example is North Lebanon, were each town recorded on average 24.58 Mumps cases over the year.
However, after Samer, his friends and a big portion of the Lebanese citizens got vaccinated against this disease, we can see the success of those vaccination campaigns in the following years (2016, 2017, and 2018) were Mumps cases gradually decreases to reach almost zero records in towns of every governorate.
Since this shows that the authorities were able to make impact in preventing and controlling outbreaks between 2015 and 2018, then they should make sure that similar measures are constantly being implemented.
Because Mumps has a negative effect on the patient’s health, and is visible in the face region which can be mentally scarring.
The approach Ministry of Public Health must take is having a preventive plan instead of a reactive one to eliminate Mumps’ outbreaks. And this can be done through a set of actions:
- Ensure ahead of time that vaccines are available at health centers before the actual date of vaccination.
- Follow closely the progress of vaccination campaigns, especially in governorates with higher tendency for outbreaks.
- Increase awareness concerning this disease and the importance of being vaccinated.
- Benefit from lessons learned in campaigns done previously for Mumps especially between the 2015-2018 period, and how outbreaks were dealt with.
Taking those recommendations along with insights from specialists in the field will allow the MoPH to ensure the safety of citizens by preventing them from such harmful diseases. This way Samer and his friends don’t have to go through this disease that is harmful physically and disturbing.

by rms106 | Nov 17, 2025 | Visualization
“ When it comes to health, your ZIP code matters more than your genetic code ” – Dr. Tony B. Iton
The Healthcare Scene in Lebanon
Rami spent the majority of his life in Aley, Choueifat El Aamrousiyeh, a quiet town where people know each other all throughout the area. When Covid-19 began spreading in Lebanon, he assumed that his location would be relatively safe in terms of health implications. After all, the news was primarily focused on Beirut.
During peak months, Rami started hearing about his neighbors testing positive at a pace he certainly did not expect. Meanwhile, his cousin Leila, who lives close by in Kahhaleh, hardly knew anyone infected. They were both in the same region, but faced entirely different risks.
Rami’s worry and stress levels grew a lot, especially for his elderly parents with chronic conditions. If Covid spread in his town at a fast pace, would they be able to get help in time? Would testing and vaccination centers be available in close proximity to where they live? Would nearby hospitals be overwhelmed with full capacities?
Leila and Rami’s experiences reflect what many Lebanese families endure. Two households in the same region, but different towns, had completely different stress levels regarding the readiness of healthcare emergency responses.
Health Patterns in Lebanon: What the Data Reveals
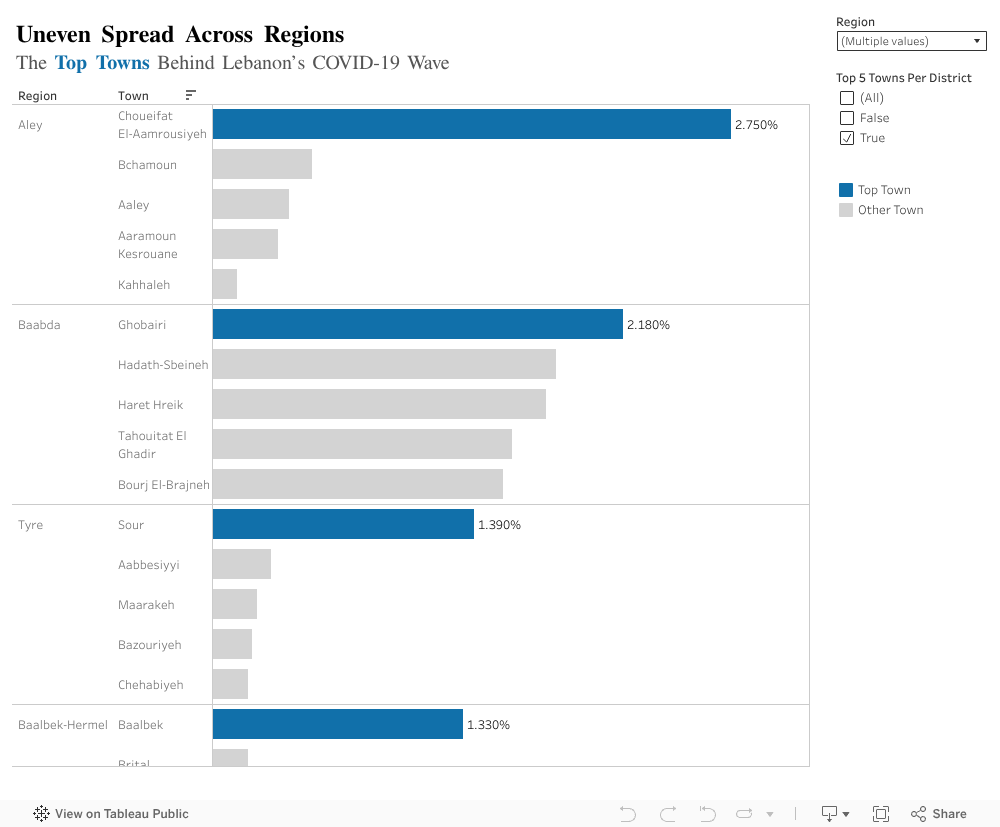
We tend to think of public health at the regional level, but covid behaved more so at a town level per region. This exposed imbalances that are not usually explored. Top town per region with the highest contribution to the total national case count revealed unexpected results:
-
- In Aley (region), Choueifat Aamrousiyeh alone accounted for 2.75% of all cases in the country.
- In Baalbek-Hermel, Baalbek alone stood out with 1.33%, which is much higher than surrounding towns.
- The remaining regions showed similar patterns: one or two towns carried the majority of cases.
What Does This Mean Exactly?
People like Rami, who happen to live in a high risk town, experienced a completely different pandemic from people in towns just a few kilometers away. This is likely to repeat in the future if another major healthcare crisis hits the country.
Moving Forward, What Can Be Done?
-
- Prioritize hotspot towns: testing centers, clinics, and awareness campaigns should start where case data shows concentration, not where population is highest.
- Build local readiness plans: Instead of generic region level plans, towns with higher infection percentages need specific preparation steps (rapid testing, temporary isolation centers, and community awareness).
- Use data driven action plans: Covid case percentages help identify where outbreaks are likely to happen again. If regions plan smarter, hospitals and clinics face less chaos.
- Strengthen communication and public awareness: Towns with consistently high rates should receive ongoing health messaging to prevent repeat scenarios.
The Key Takeaway
By understanding how Covid-19 was not distributed proportionately across towns, we can finally design smarter, more effective responses. This applies not only to pandemic/epidemics, but to any future public health threat in Lebanon.