Unequal Support: When Small Numbers Hide Real Lives
This is Jane, a 27-year-old Ethiopian domestic worker living in Akkar.
Last month, when she got sick, she had no access to community aid, legal protection, or medical support.
She waited four days before anyone could help her—not because support didn’t exist, but because in Akkar there are too few immigrant workers to be considered a priority.
Jane’s struggle is not personal—it’s structural.
Immigrant workers in Lebanon are not distributed evenly across the country, and when population numbers are small, support systems disappear.
Small communities become invisible, unheard, and unprotected.
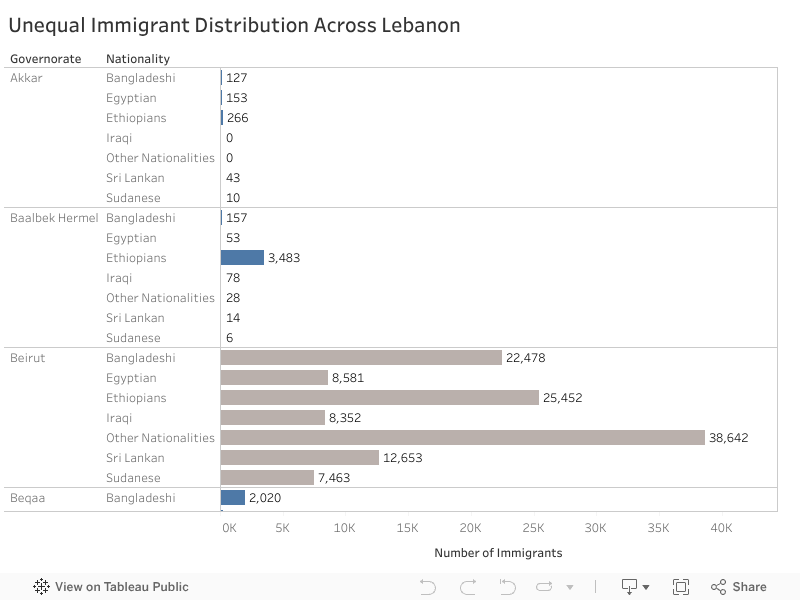
Below is the distribution of immigrant workers across Lebanon by nationality and governorate.
Everything in blue represents a community with fewer than 10,000 workers, meaning low visibility and often no access to essential support.
While Beirut hosts extremely large populations — for example 38,642 workers labeled “Other Nationalities” and 25,452 Ethiopians—governorates like Akkar host only 266 Ethiopians and 127 Bangladeshis.
Yet behind every small number is a real human life.
If We Do Nothing
If nothing changes, workers like Jane will continue to suffer in silence.
Low-population regions will remain overlooked, and inequality will deepen — not because help doesn’t exist, but because help isn’t distributed fairly.
What Can We Do?
Solution 1—Mobile Clinics
Mobile clinics are medical vans that travel to underserved regions to deliver basic healthcare.
They bring support to people who cannot safely or affordably reach Beirut.
During COVID-19, NGOs in Lebanon successfully used mobile medical units to reach remote areas — proving that mobility overcomes geographic inequality.
Solution 2—Rotating Outreach Teams
Teams of legal advisors, translators, and social workers rotate across governorates weekly, providing education, protection, and emergency help.
This approach already works in Jordan, where outreach teams support Syrian refugees in dispersed rural camps without needing permanent offices.
Solution 3—Minimum-Support Policies
A national guarantee ensuring every governorate receives a basic level of support, regardless of population size.
Just as Lebanon provides schools, electricity, and hospitals to small villages, immigrant workers deserve equal dignity and safety.
Findings & Recommendation
Support should not depend on population size — dignity must be universal.
Lebanon should adopt minimum-support policies, expand mobile and rotating services, and ensure that no worker is invisible.
Access to healthcare in Lebanon depends on one simple but critical factor: where you live. But until you visualize the distribution of facilities across the country, it’s hard to truly see how unequal that access is.
I started this project by aggregating six types of health facilities — hospitals, clinics, medical centers, pharmacies, labs and radiology centers, and first-aid centers — across all districts using the PKGCube Health Resources dataset. After cleaning and restructuring the data, one pattern immediately stood out: Lebanon’s map of healthcare is far from balanced.
To understand this more clearly, I built a district-level visualization and redesigned it using explanatory design principles. And once the noise was removed, the picture became unmistakable.
The Key Insight
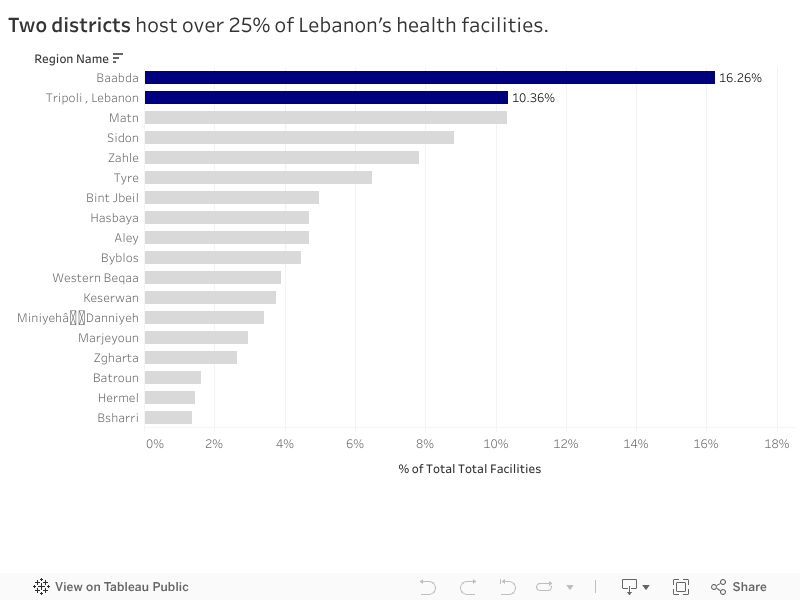
Two districts — Baabda and Tripoli — hold more than a quarter of all health facilities in the entire country. Just two.
Meanwhile, at the opposite end, districts like Hermel and Bsharri combined account for less than 3%.
In a country with major infrastructure gaps and uneven population distribution, this imbalance has consequences:
It shapes how far people travel to access care.
It affects waiting times, congestion, and referral patterns.
And in crisis situations, it determines who gets help quickly and who doesn’t.
The redesigned visualization highlights this story intentionally. The top two districts are shown in strong blue, while the rest of the country fades into context. No clutter, no distractions — the contrast lets the insight speak for itself.
What It Means
This distribution doesn’t automatically mean Baabda and Tripoli are “over-resourced” or that Hermel and Bsharri are “neglected.” Counts are not the same as capacity, staffing, or service quality.
But the numbers do reveal something important: If health planning is meant to be equitable, we can’t treat all districts as if they start from the same baseline.
Policymakers and NGOs could use these insights to:
Prioritize new facility investment in low-share districts
Support underserved areas with mobile clinics or telehealth units
Track whether the distribution becomes more or less concentrated over time
What Comes Next
This visualization is a starting point. The next step is to connect the facility distribution with:
District-level population
Accessibility and travel time
Facility capacity indicators
That is when the story becomes more than a map — it becomes a tool for planning.
For now, the message is simple: Lebanon’s health infrastructure is unevenly distributed, and two districts carry a disproportionate share of the country’s access.
In Lebanon, access to healthcare can change drastically with geography. A person in Tripoli can find a clinic or pharmacy on nearly every corner, while someone in Hermel or Zahleh might travel hours for the same care.
Using data obtained from the AUB Linked Open Data Portal, I explored how healthcare facilities are distributed across more than 1,100 Lebanese towns. The goal was to understand whether medical services are spread evenly across the country or concentrated in only a few locations.
Uneven Access Across Towns
The data reveals a clear imbalance. Healthcare services are heavily centralized in urban areas, particularly Tripoli, Saida, and Haret Hreik, which together host the largest share of Lebanon’s medical facilities.
Tripoli alone has more than 230 healthcare establishments, while dozens of smaller towns have fewer than 20 facilities, and some have none at all.
This concentration means that people living in rural and inland areas often need to travel long distances for even basic medical services, while urban hospitals and clinics struggle with overcrowding and high patient loads.
It highlights a system where location determines opportunity, where healthcare is available not based on need, but on proximity to major cities.
What Kinds of Facilities Exist?
When we look at the types of healthcare facilities, pharmacies and clinics dominate the landscape. They make up the majority of Lebanon’s healthcare infrastructure, far outnumbering hospitals and specialized centers.
While pharmacies and small clinics ensure access to medication and consultations, hospitals and diagnostic centers are much fewer, especially outside major cities. This shows a healthcare system that leans more on treatment through medication than on preventive or emergency care.
Balancing the Map: How Geography Shapes Access
Together, these findings reveal how geography continues to shape healthcare opportunities in Lebanon. The concentration of facilities in urban centers not only affects access but also contributes to inequalities in health outcomes. Urban residents have quicker access to doctors, specialists, and emergency units, while rural populations often rely on limited local clinics or travel hours to reach adequate care.
These patterns underline the urgent need for balanced healthcare investment. Rural areas require new clinics, laboratories, and emergency units that bring services closer to people’s homes. Improving healthcare equity is not only a matter of infrastructure, it’s about ensuring that every Lebanese citizen, regardless of location, can access timely, reliable care.
Final Reflection
This analysis shows how data visualization can make inequality visible. By mapping and quantifying healthcare access, we can move beyond perception and use data to guide smarter, fairer policy decisions. Ultimately, every dataset tells a story, and in this one, the message is clear:
“Health should not depend on your zip code.”
Tags: healthcare, Lebanon, inequality, data visualization, open data, AUB