by ima46 | Nov 21, 2025 | Uncategorized
It was a quiet Sunday afternoon in a small town in the West Bekaa. Two friends, Jad (15) and Rami (14), were enjoying a simple innocent motor bike ride. But unfortunately, they were hit by a speeding SUV.
The town folk gathered around the 2 boys that were laying bleeding on the asphalt road. The ambulance arrived quickly. Jad needed immediate, high-level trauma care. He needed a specialized surgeon within minutes. The nearest facility capable of saving his life, however, was in Zahle, a 45-minute drive through challenging rural roads.
For severe trauma, 45 minutes is not a journey, but it is a critical time window that determines fate. While Rami survived after weeks in the ICU, Jad unfortunately bled out on the way.
His death wasn’t solely a result of the collision. But it was a devastating consequence of a systemic, geographical failure.
The Evidence: Mapping the Disparity
This tragedy is not an isolated incident of bad luck. It is the human cost of a deeply imbalanced healthcare system. Our data analysis confirms what rural families already know: Access to care is dangerously centralized.
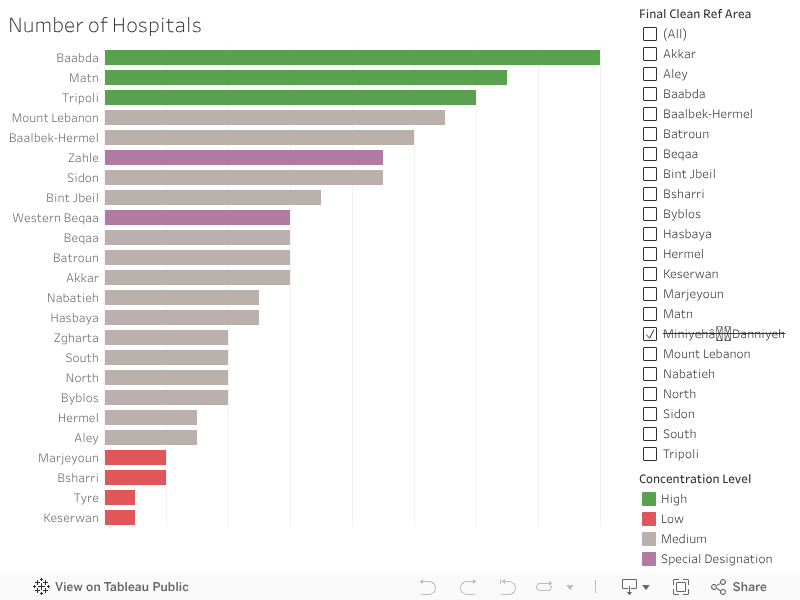
The visualization of medical facilities across Lebanon’s districts illustrates this shocking disparity:
-
The areas highlighted in Green (the top 3) enjoy a dense concentration of hospitals, offering multiple lifelines within minutes.
-
On the opposite end, the areas highlighted in Red (the bottom 4) show bars that are barely visible, confirming these are healthcare deserts.
The system is designed to serve the city, leaving the vast rural expanse with an inadequate margin of error. Your chance of survival is, quite literally, dictated by the proximity of your nearest bar on this chart.
The Solution
We cannot solve the problem of distance by trying to build a new university medical center in every district. That is fiscally impossible. The real solution is smart, targeted investment in stabilizing the patient, not relocating the hospital.
Our data, which shows the alarmingly low density of First Aid and Care Units in the rural areas, points directly to the answer. We must transform these simple clinics into advanced, highly efficient units.
1. Buying Time
The difference between life and death for someone like Jad is the critical time immediately following a severe injury.
The goal of a new, Trauma-Ready Care Unit is to manage and stabilize major injuries (like severe bleeding or airway obstruction) for 30 minutes. It’s not a full operating room, but it has the specialized staff and equipment to:
By creating these small hubs, we effectively shrink the deadly 45-minute travel time into a manageable window, giving the patient the chance to survive the journey to the major hospital.
2. Decompressing the ER
The benefits flow both ways. Today, emergency rooms in major urban hospitals (like those in Zahle or Baabda) are often jammed with non-critical cases:
By upgrading rural units, these facilities can handle this high volume of urgent but non-life-threatening cases.
The immediate effect is a massive reduction in pressure on the urban ERs. This allows the major city hospitals to focus their specialized surgeons and resources entirely on the true, severe emergencies, like the trauma case that should have saved Jad.
Big Idea: “Healthcare equality is not just about bringing care closer; it’s about making sure the right care is available at the right time for everyone, everywhere.” Investing in these small, advanced units is the fastest, most cost-effective way to bridge the deadly gap on our map.

by zct01 | Nov 21, 2025 | Uncategorized
A Morning in Akkar
Somewhere in the hills of Akkar, a mother wakes before dawn. Her son is burning with fever, his tiny chest rising in short, frightened breaths.
She wraps him in a blanket, steps outside and faces the same impossible truth every family in her town lives with:
There is no clinic here.
No doctor.
No nearby care.
The closest medical help is more than an hour away—if roads are clear, if transportation can be found, if nothing goes wrong. For her, and for nearly half of Lebanon’s towns, simple illnesses can become life-threatening journeys. It is not just a healthcare issue, It is a daily, silent tragedy that shapes entire lives.
What the Data Shows but the Country Ignores
The visuals map this tragedy with painful clarity.
In the bar chart:
-
49.74% of Lebanese towns have no local resources nor nearby healthcare.
-
17.08% have no local facilities but can sometimes reach distant care.
Only 33.19% enjoy the basic dignity of accessible treatment.
The map shows Lebanon carved into colors that reveal the geography of abandonment.
-
Akkar, North Lebanon, Baalbek-Hermel, and Bekaa glow in urgent shades of red.
-
Beirut and Mount Lebanon rest confidently in green.
-
Though South Lebanon contains the highest danger percentage, it is covered with governorates that contain abundant amount of medical facilities and resources.
The visuals prove what families in rural regions already know: healthcare access in Lebanon is not just unequal—it is deeply, structurally unfair.
The danger zones are not random, they follow the borders of poverty, neglect, and distance.
A Country at a Crossroads
Yet Lebanon is not without hope. Around the world—and even within its own borders—innovative models show that remote and underserved communities can receive consistent care. The country stands at a crossroads where solutions are known, feasible, and within reach.
Lebanon can choose a future where no mother must gamble with her child’s life because of distance.
That future begins with a hybrid healthcare access model designed for real Lebanese terrain, real Lebanese families, and real Lebanese limitations.
Building the Path Forward
The path unfolds in two phases—immediate relief and lasting transformation.
Immediate Relief
-
Mobile clinics traveling weekly into remote towns.
-
Telehealth services connecting residents with doctors online.
-
Community health workers offering first aid, monitoring chronic diseases, and stabilizing emergencies.
These solutions bring healthcare to the people, rather than asking the people to chase it.
Long-Term Transformation
-
Expanding rural Primary Healthcare Centers (PHCs) in governorates painted red in the danger map.
-
Incentivizing private and nonprofit partnerships to open satellite clinics.
-
Improving transportation links so that even without a local clinic, emergency care is reachable.
This approach does not just fill gaps, it builds a system where every town becomes medically reachable, no matter how far, no matter how rural.
Why This Will Work
Proof already exists.
Organizations like MSF, the Lebanese Red Cross, and multiple NGOs have successfully delivered mobile and remote care across Lebanon’s hardest-to-reach regions. Telehealth has grown worldwide, saving millions in rural communities and the data that drives these charts, maps, and analyses pinpoint exactly where interventions must be prioritized.
The strategy aligns with Lebanon’s national health vision and mirrors international best practices in countries with similar geography and instability.
It is not theory.
It is tested, validated, and realistic.
Beyond the Diagnosis
The visuals do not simply highlight shortages, they illuminate where change must begin.
The Truth
-
Lebanon’s healthcare inequality is regional and predictable, not accidental.
-
Rural northern and eastern regions are in critical danger, lacking both local and nearby care.
-
Nearly half of Lebanese towns face severe accessibility barriers.
The Solution
-
Deploy mobile and telehealth clinics immediately to stabilize high-danger governorates.
-
Invest in long-term PHC expansion to ensure durable access.
-
Integrate transportation and healthcare planning, recognizing that distance is often deadlier than disease.
-
Maintain data-driven monitoring to continuously reallocate resources to evolving needs.
If Lebanon acts now and not later, the red zones can fade. Families can breathe easier. Lives can be saved.
A Different Dawn
One day, perhaps, a child in Akkar will still wake before dawn—but instead of gasping for breath, he will leap from bed to greet a new school day. His mother will no longer fear the distance to care.
Because care will finally be within reach. Because the map will no longer define who survives and who struggles. Because Lebanon will have remembered its forgotten towns.
That is the story the data tells. That is the story this country can still rewrite.
“We are alive the most when we are faced with adversity like no other.”

by mms90 | Nov 21, 2025 | Uncategorized, Visualization
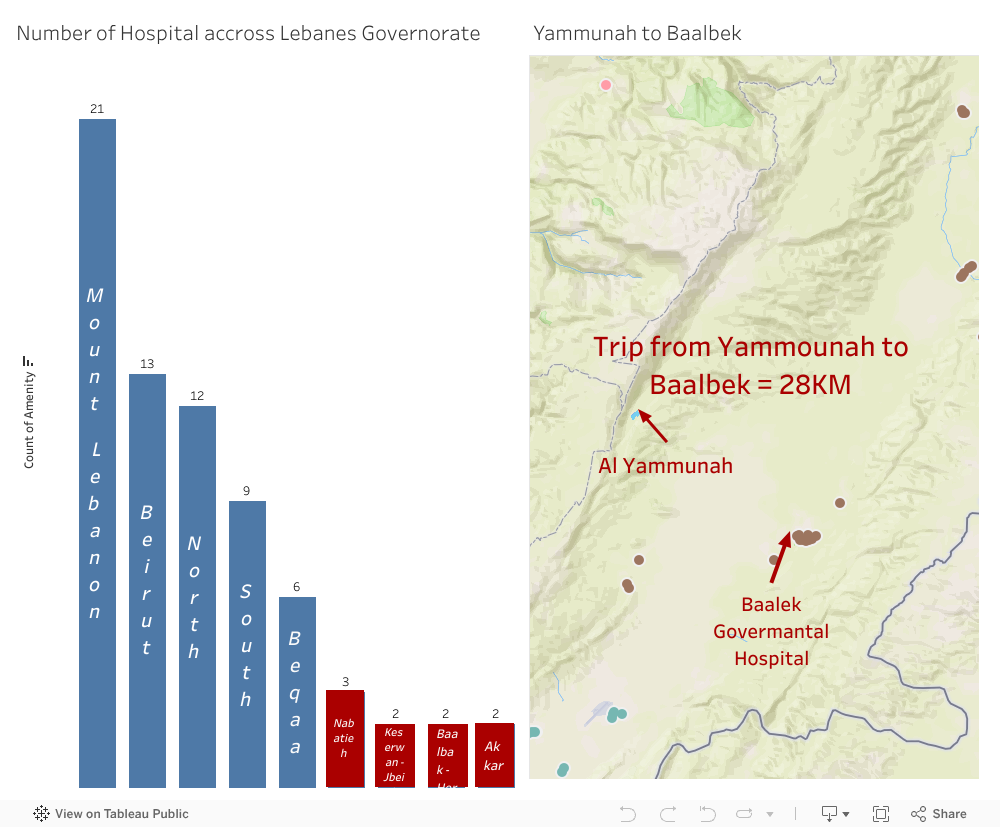
Farid’s weekly trip from Yammoune shows how distance can stand between a patient and lifesaving care.
“For many in rural Lebanon, the first battle isn’t the illness—it’s the road.”
Farid’s weekly journey
Farid lives in Yammoune, a mountain village in the Beqaa (Baalbek District). He travels to the nearest hospital about 28 km away, a trip that takes roughly 40–45 minutes—and he does this two to three times a week for cancer treatment. The drive, the weather, and the rough roads make every visit heavy and exhausting
The geography problem
Rural communities in Lebanon face long distances to care, limited transport options, and winter closures on mountain roads. When the nearest hospital is far, time lost on the road can mean care delayed, especially for urgent cases like chemotherapy, dialysis, emergencies, or childbirth.
“Every kilometer matter, especially when minutes do too.”
Why nearby hospitals matter
- Faster treatment: Shorter trips mean earlier interventions and fewer missed appointments.
- Less strain on families: Reduced travel costs and stress for caregivers.
- Health equity: Brings rural patients closer to the standard of care found in cities.
- System resilience: Local facilities ease congestion at major urban hospitals.
What we can do
- Invest in satellite oncology units and urgent care centers in rural hubs.
- Strengthen referral networks so stabilization happens locally before transfers.
- Mobile clinics & telehealth to bridge gaps while facilities are built.
- Reliable transport support (subsidized rides/ambulances) for critical patients.
- Data-driven planning to prioritize locations with the highest access gaps.
A human ask
Farid’s story is not unique. For patients like him, a nearby hospital isn’t just convenience, it’s dignity, energy, and a real chance to keep fighting.

by Sara Dabbous | May 7, 2020 | Dashboard, Visualization
Since I started working in the healthcare sector I’ve always been interested in knowing more about this industry. As such, while exploring the WDI Data I studied several healthcare indicators and it turns out – Lebanon is doing better than we thought! I was intrigued to know what’s beyond those indicators, and luckily I found a detailed dataset about Primary Health Care Centers in Lebanon on The Humanitarian Data Exchange, I was surprised to know we had this many centers.
Could this visualization be a sign of a sound healthcare system ?
Did this awareness in healthcare aid us in containing the Covid-19?
Do you think there is a better future for the healthcare system for Lebanon, or will it be worst?
Personally, I am optimistic..
So here are some things I didn’t know:
- There are 174 Operational Primary Healthcare Centers in Lebanon
- There are 25 PHC funded by UNHCR
- There are 100 PHC that provide subsidized services.
- Nabatieh has 0 operational PHCs.
- The North governorate has the highest number of operational PHC: 36

In this dashboard, I prepared – using Tableau – a map that shows the different Operational PHC locations in Lebanon filtered by UNHCR Funding. Alongside it, is a bar chart showing the percentage of operational PHC in each Governorate. Finally, at the bottom, you can find a stacked bar chart representing the number of operational PHC per governorate, highlighting those who offer subsidized services.