by wge06 | Nov 28, 2025 | Uncategorized
Beyond the Waiting Room: Revealing “Invisible” Patients of an NGO
By: Nivine Manasfi, Wissam El Sabeh, Yasmina El Dirani, Hussein Charafeddine, and Perla Abou Rjeily
In humanitarian aid, success is often measured by volume. For the Imam Sadr Foundation (ISF), 31,430 patient visits over two years suggested a thriving system. However, our deep-dive analysis revealed that aggregate numbers were hiding a “silent crisis” of missing patients.
To understand why these groups were missing, we didn’t just look at the records—we asked the community. Here is how our impact survey validated the data and shaped our solutions.

1. The Gender Gap: It’s About Work, Not Health
Data showed a stark imbalance: 67% of patients were female, while only 33% were male. Our survey revealed the structural cause:
The Fix: We proposed launching “Evening Clinics” (5 PM – 8 PM) to capture the working demographic that the current schedule excludes.

2. The Mental Health Stigma
Despite high trauma levels in the region, Syrian refugees accounted for near-zero mental health visits. The survey confirmed that stigma is the primary barrier:
-
62% of patients cited “privacy and secrecy” as the main reason they avoid seeking mental health support.
-
Integrating mental health screenings into general medical visits was the 3rd highest requested service improvement.
The Fix: By integrating mental health checks into standard intake forms, clinics can bypass the “psychotherapy” label that scares patients away.

3. Neglecting Prevention
Preventive services (like vaccination and dental) made up less than 1% of total visits. However, the survey proved this isn’t due to a lack of interest:
The Fix: The demand exists. We recommended strengthening the preventive infrastructure and using doctors, rather than just nurses, to drive awareness during standard consults.
Conclusion
Analyzing the dataset turned “records” into insights, but the survey turned that insights into action. By shifting our focus from volume of visits to equity, we proved that true healthcare success isn’t just about how many people you serve—it’s about ensuring no one is left invisible.

by rms106 | Nov 17, 2025 | Visualization
“ When it comes to health, your ZIP code matters more than your genetic code ” – Dr. Tony B. Iton
The Healthcare Scene in Lebanon
Rami spent the majority of his life in Aley, Choueifat El Aamrousiyeh, a quiet town where people know each other all throughout the area. When Covid-19 began spreading in Lebanon, he assumed that his location would be relatively safe in terms of health implications. After all, the news was primarily focused on Beirut.
During peak months, Rami started hearing about his neighbors testing positive at a pace he certainly did not expect. Meanwhile, his cousin Leila, who lives close by in Kahhaleh, hardly knew anyone infected. They were both in the same region, but faced entirely different risks.
Rami’s worry and stress levels grew a lot, especially for his elderly parents with chronic conditions. If Covid spread in his town at a fast pace, would they be able to get help in time? Would testing and vaccination centers be available in close proximity to where they live? Would nearby hospitals be overwhelmed with full capacities?
Leila and Rami’s experiences reflect what many Lebanese families endure. Two households in the same region, but different towns, had completely different stress levels regarding the readiness of healthcare emergency responses.
Health Patterns in Lebanon: What the Data Reveals
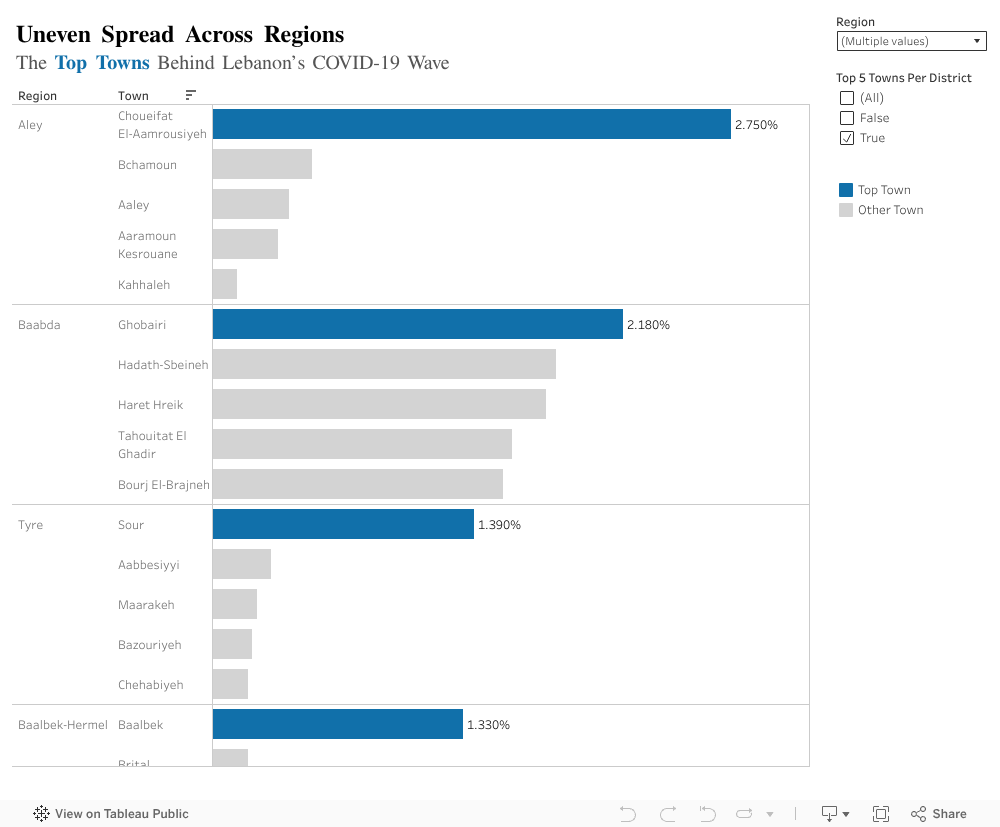
We tend to think of public health at the regional level, but covid behaved more so at a town level per region. This exposed imbalances that are not usually explored. Top town per region with the highest contribution to the total national case count revealed unexpected results:
-
- In Aley (region), Choueifat Aamrousiyeh alone accounted for 2.75% of all cases in the country.
- In Baalbek-Hermel, Baalbek alone stood out with 1.33%, which is much higher than surrounding towns.
- The remaining regions showed similar patterns: one or two towns carried the majority of cases.
What Does This Mean Exactly?
People like Rami, who happen to live in a high risk town, experienced a completely different pandemic from people in towns just a few kilometers away. This is likely to repeat in the future if another major healthcare crisis hits the country.
Moving Forward, What Can Be Done?
-
- Prioritize hotspot towns: testing centers, clinics, and awareness campaigns should start where case data shows concentration, not where population is highest.
- Build local readiness plans: Instead of generic region level plans, towns with higher infection percentages need specific preparation steps (rapid testing, temporary isolation centers, and community awareness).
- Use data driven action plans: Covid case percentages help identify where outbreaks are likely to happen again. If regions plan smarter, hospitals and clinics face less chaos.
- Strengthen communication and public awareness: Towns with consistently high rates should receive ongoing health messaging to prevent repeat scenarios.
The Key Takeaway
By understanding how Covid-19 was not distributed proportionately across towns, we can finally design smarter, more effective responses. This applies not only to pandemic/epidemics, but to any future public health threat in Lebanon.

by thm14 | Nov 20, 2023 | Uncategorized
A Beacon of Hope for the Patients in Lebanon
This does not start with a funny caption or a happy anecdote, but I assure you it’s an important topic and it touches the lives of everyone. This is Tarek Moukalled, and I hope that by the end of this session you can see the light at the end of the tunnel for patients in Lebanon.
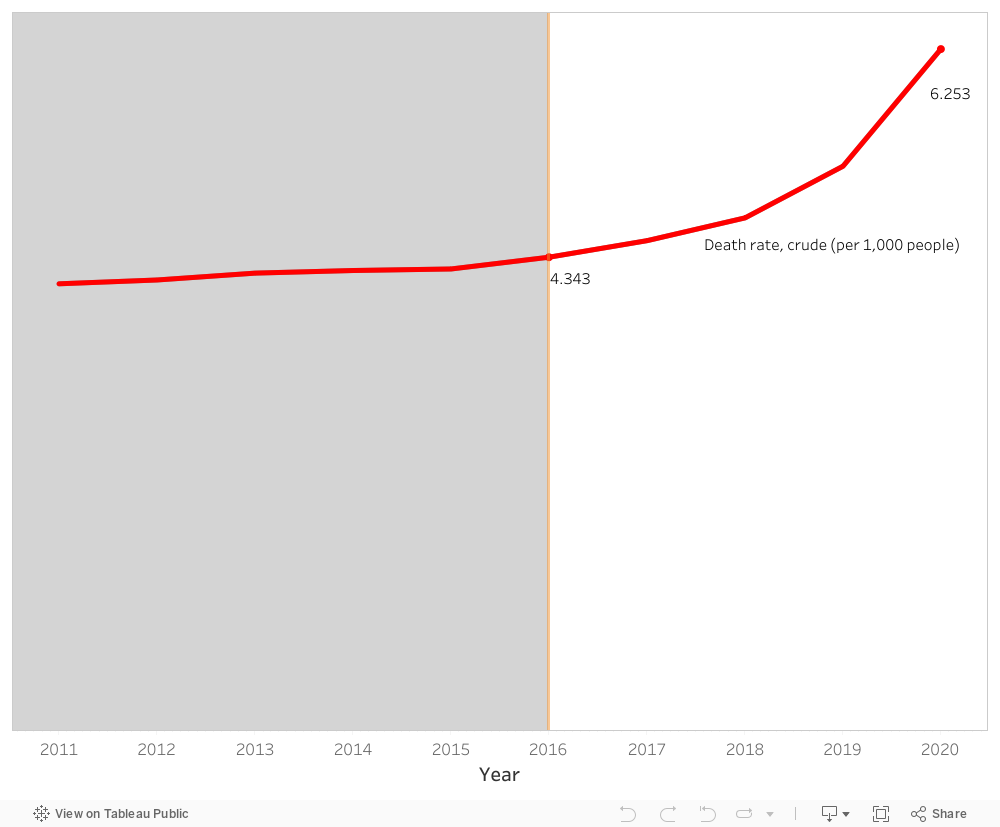
Our story begins with rather an unfortunate observation. Patients in Lebanon are dying. As a matter of fact, the death rate has increased from 4.34 deaths in 2016 to 6.25 deaths in 2020 per 1,000 persons. That is drastic and an alarming increase of approximately 44 % during a span of 5 years. But why?
A close inspection of the healthcare expenditure per capita during the suggested years shows a considerable increase from 648 USD to 995 USD. Furthermore, the % expenditure of GDP on healthcare in Lebanon also shows a consistent trend of a little less than 8 % across the same years. So, things should be fine, if not better! Yet unfortunately, this is not the case.
It appears the Lebanese people have been taking things into their hands. With the economic recession and the subsequent governmental bankruptcy, GDP decreased from ~ 51.1 billion USD in 2016 to 31.7 billion USD in 2020. This led to the fact that the Lebanese people have been paying more and more from their own pockets for healthcare reaching a whopping 44.2 % of healthcare expenditure in 2020.
Comparing the above results with the healthcare sector of a different country that shares similar demographics and healthcare expenditure with Lebanon would help with the context and the subsequent validation of the proposed solution, the light at the end of the tunnel. Remember?
With a similar % expenditure of GDP on healthcare (~ 7.5 %) and a little lower starting point in death rate of 3.16 per 1,000 persons, Jordan’s death rate in 2020 reaches 3.47 per 1,000 persons. The healthcare expenditure per capita in Jordan is consistently way lower than that of Lebanon. The % of out-of-pocket expenditure on healthcare is also steady and lower than that of Lebanon. As to the GDP, it starts lower than Lebanon in 2016 at ~ 39.9 billion USD and ends higher than Lebanon at 43.6 billion USD. As such, the main considerable deviation between both countries is the GDP amount. For that matter, it’s important to note that economies and healthcare sectors grow through expenditure rather than stagnation or restriction.
The increase in the share of health expenditure as part of GDP will have positive results on both short-term and long-term.
- Enhanced Healthcare Quality
- Faster Healthcare Response
- Improved Patient Health Outcome
- Decreased Death Rate
- Target for Healthcare Tourism
With that, it is imperative to urge whoever who is responsible to proceed with the increase in healthcare expenditure for the sake of our patients and our future.
Thank You

by aab75 | Nov 18, 2023 | Visualization
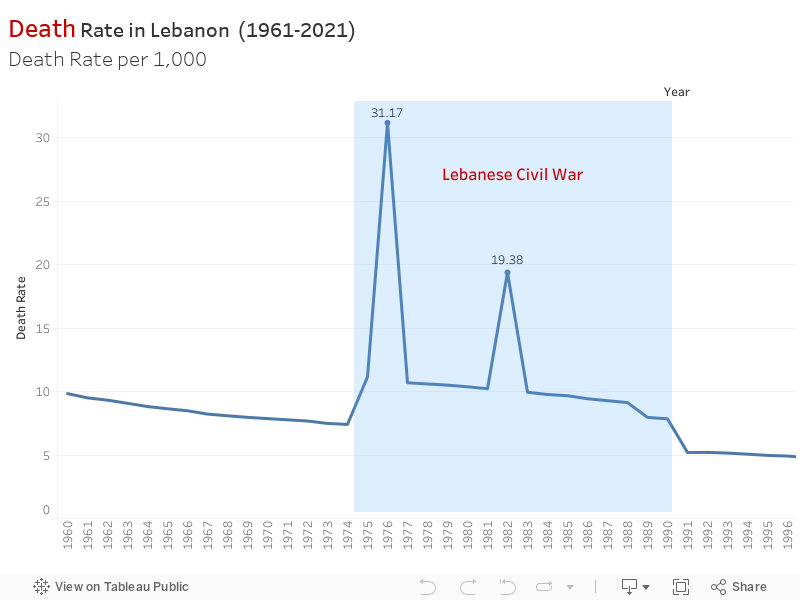
In light of recent events, we delved into a pressing issue: the unsettling fluctuations in mortality rates in Lebanon. It was evident that these shifts had deeper roots, impacting lives and reflecting significant historical events.
The data painted a stark picture. Between 1975 and 1990, Lebanon witnessed a devastating surge in mortality rates, reaching a staggering 31.17. The Lebanese Civil War cast a long shadow, leaving behind a legacy of loss and devastation that echoed in the mortality records.
Post-1990, there was a semblance of stability with mortality rates hovering around 4-5, despite intermittent spikes like the one in 2006 during the July War. It seemed like a fragile peace amid lingering echoes of conflict.
Then, at the dawn of 2019, another dramatic shift occurred. The onset of the COVID-19 pandemic jolted mortality rates sharply upward once more. It was a distressing reminder of how swiftly external factors could disrupt the delicate balance of life.
Contribution to SDG
SDG 3: Good Health and Well-being: The significant increase in mortality rates during the Lebanese Civil War, subsequent fluctuations due to regional conflicts like the July 2006 war, and the sharp increase attributed to the COVID-19 pandemic highlight the importance of SDG 3. It emphasizes the need for resilient healthcare systems, disease prevention, and access to quality healthcare, especially during periods of conflict and health crises.
SDG 16: Peace, Justice, and Strong Institutions: The impact of the Lebanese Civil War and regional conflicts on mortality rates underscores the relevance of SDG 16. Ensuring peace, stability, and strong institutions is vital to prevent the adverse effects of conflicts on public health and to establish systems capable of effectively managing crises and their aftermath.
SDG 10: Reduced Inequalities: The fluctuations in mortality rates due to historical conflicts and the COVID-19 pandemic might reveal disparities and inequalities in healthcare access, response, and resilience. Addressing SDG 10 involves reducing these disparities, ensuring equitable access to healthcare services, and mitigating the disproportionate impacts of crises on vulnerable populations.