HIV persists as a noteworthy communicable disease in Europe and a substantial risk in the Arab world, posing a significant health challenge. This infection is associated with considerable healthcare costs for treatment and care, a noteworthy mortality rate, and a reduction in life expectancy. The virus specifically attacks the immune system, resulting in a persistent and severe illness with an extended incubation period before symptoms manifest.
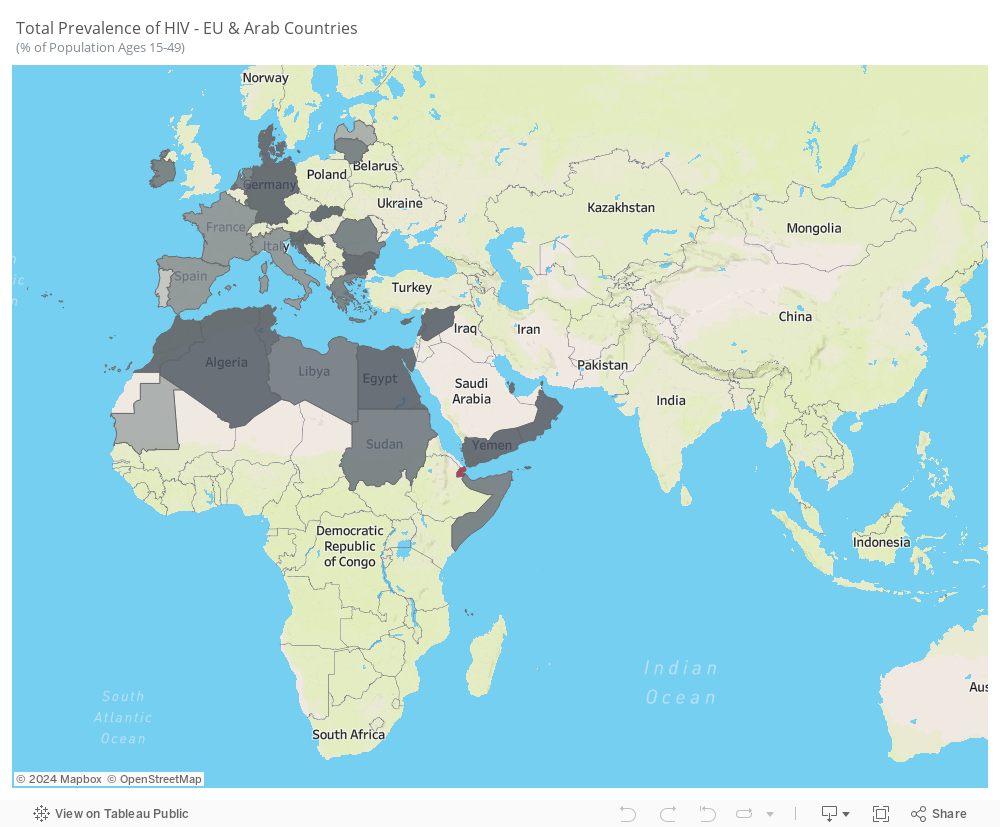
The average prevalence from 2005 to 2021 reveals notable trends. While some Arab countries, like Saudi Arabia, UAE, and Iraq, do not consistently report HIV statistics, the available data highlights the prevalence of the disease in Arab countries situated in Africa. In contrast, European countries, particularly Portugal, Latvia, France, and Italy, exhibit higher prevalence rates.
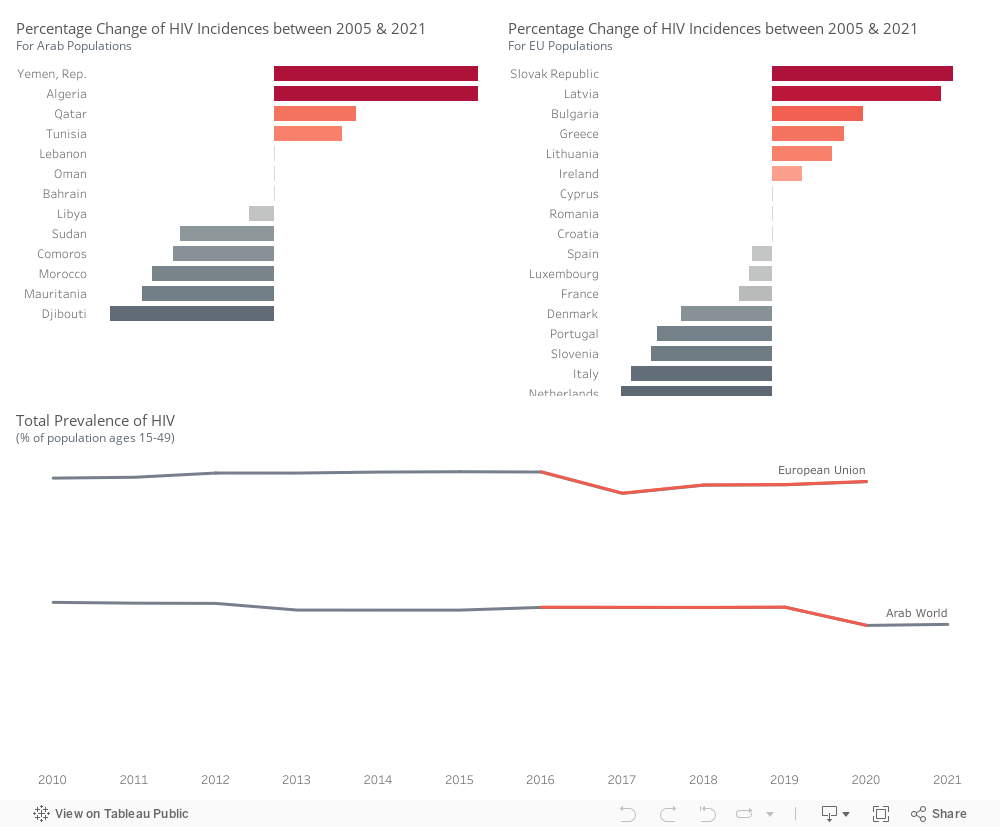
Within the Arab world, there is an upward trend in the percentage of HIV incidences in Yemen, Algeria, Qatar, and Tunisia. Conversely, Djibouti, Mauritania, Morocco, Comoros, Sudan, and Libya exhibit a decline in HIV incidence rates.
Within the Euro area, there is an increase in HIV incidences observed in Slovakia, Latvia, Bulgaria, Greece, Lithuania, and Ireland. However, a decrease is noted in the Netherlands, Italy, Slovenia, Portugal, Denmark, France, Luxembourg, Spain, and Croatia.
HIV prevalence is higher in European Union countries compared to Arab countries. There was an incline in Arab countries around 2020, while in the European Union, the trend experienced a decrease in 2017, followed by a slight upward movement.
We will be focusing on these countries in the following visuals.
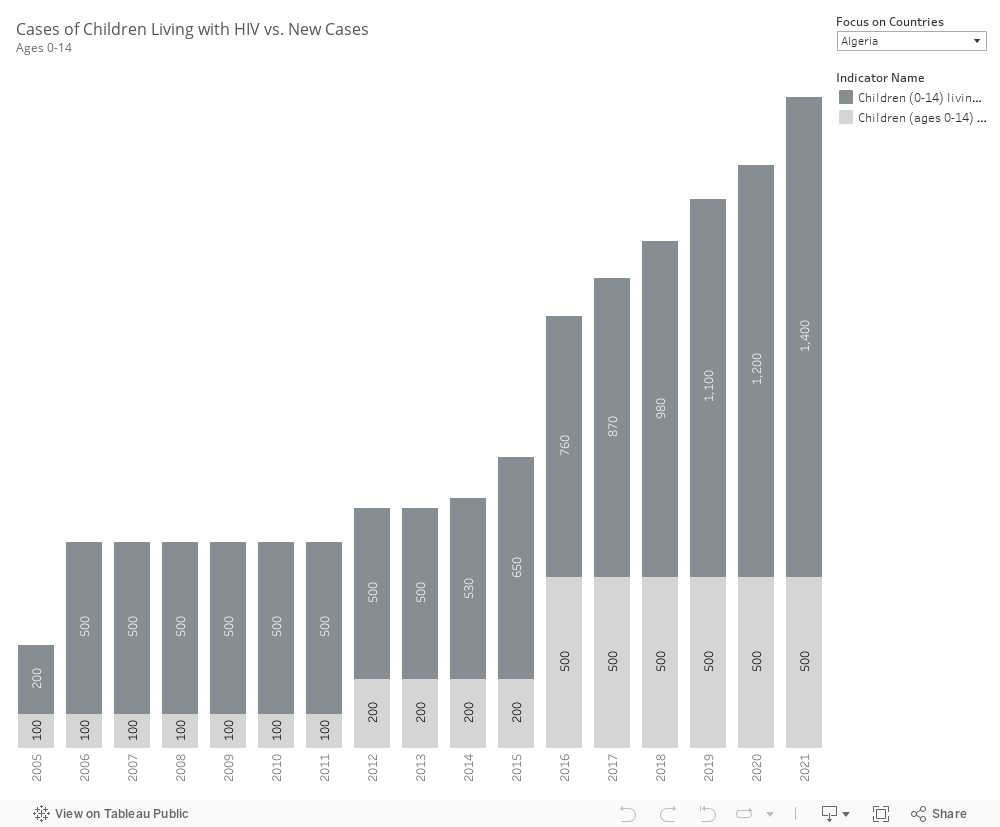
Most countries do not report parameters related to children living with HIV and newly infected children. However, the available data indicates that in Algeria and Morocco, both the number of children infected and the number of new cases are on the rise. In contrast, Djibouti has successfully decreased these numbers, as has Mauritania.
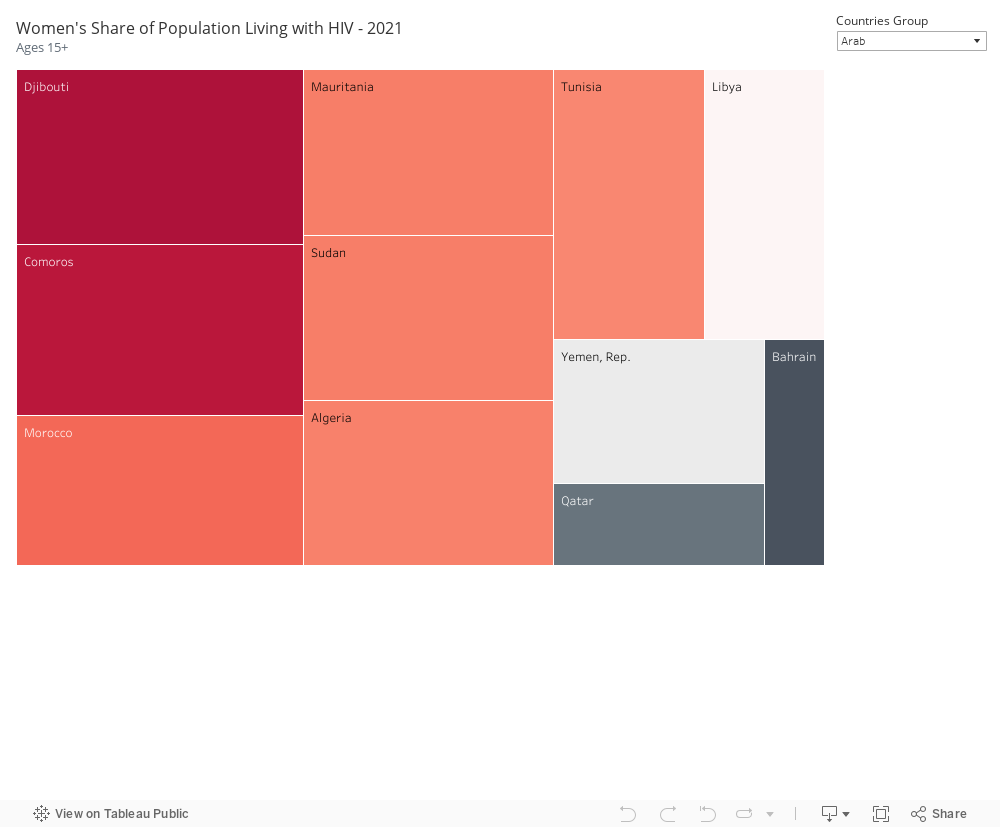
In our selected focus countries, notable instances of HIV infection among the female population are observed. Within Arab countries, Djibouti, Comoros, Mauritania, Sudan, Morocco, Algeria, and Tunisia exhibit a high prevalence. Similarly, in EU countries, France, Portugal, Latvia, Ireland, Luxembourg, and Italy show a high number of females infected with HIV.
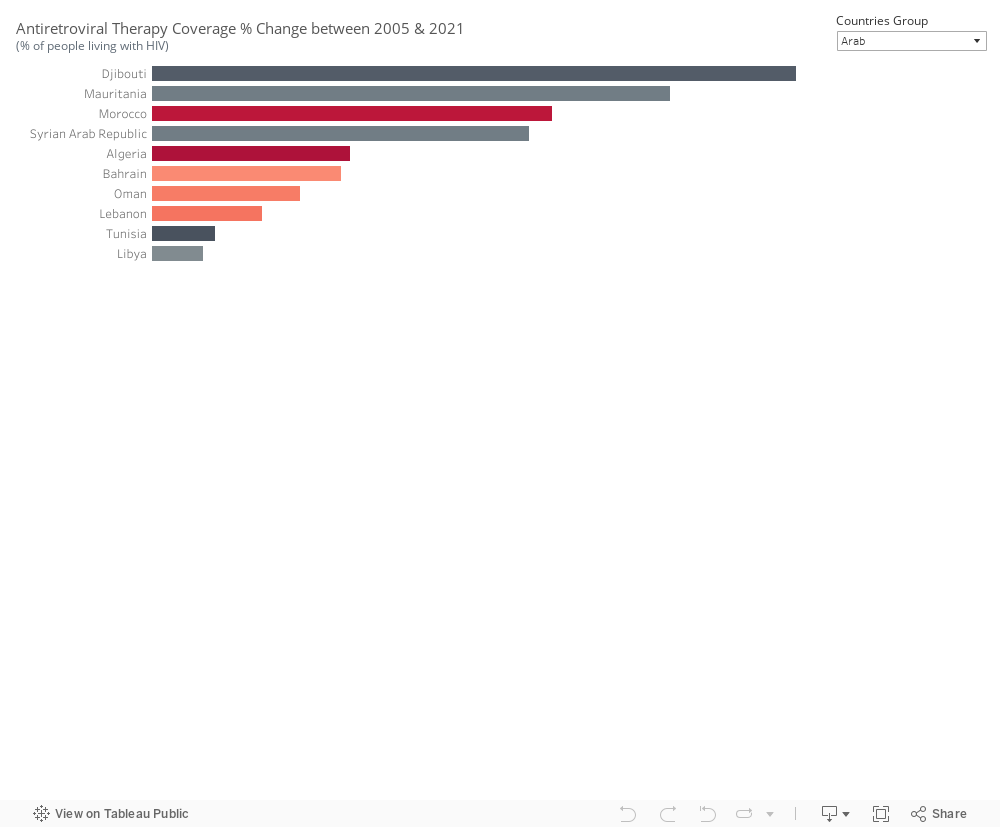
Antiretroviral therapy coverage has seen an increase since 2005 in Djibouti, Mauritania, and Morocco within the Arab world, as well as in Latvia and Bulgaria. The effectiveness of the treatment is reflected in the declining incidence cases observed. However, in Algeria, despite an increase in treatment coverage, the number of incidents continues to rise. A similar situation is noted in Slovenia, suggesting that the treatment alone may not be sufficient to curb the spread of HIV.
Information pertaining to condom use and protected sex is currently unavailable, emphasizing the need to gather this specific dataset.
In conclusion, Europe & the Arab World are far from meeting global HIV targets. Annual new HIV infections from AIDS-related illness are on the rise. While treatment can contribute to reducing the prevalence of HIV in a country, it is just one aspect of a comprehensive approach. Relying solely on treatment is inadequate. Nations should prioritize addressing other impactful factors, including:
Implementing prevention programs that effectively reach key populations in substantial numbers.
Making special efforts to enhance and extend HIV testing and treatment initiatives.
Increasing engagement with the younger demographic.
Enforcing effective policies such as mandatory testing for work or residence permits, mandatory testing for marriage, and criminalizing activities such as sex work and drug use or possession for personal use.
In the wake of economic crises that shook nations, Lebanon in 2019 and Greece in 2010 faced turbulent times. Both crises were rooted in corruption, leading to drastic declines in GDP growth. However, the divergent paths they took in managing their public health expenditures reflected the crucial role of external support, particularly from the European Union (EU), in shaping their healthcare resilience. The following graph depicts the impact of each economic crisis on the growth of the GDP for each country.
Greece:
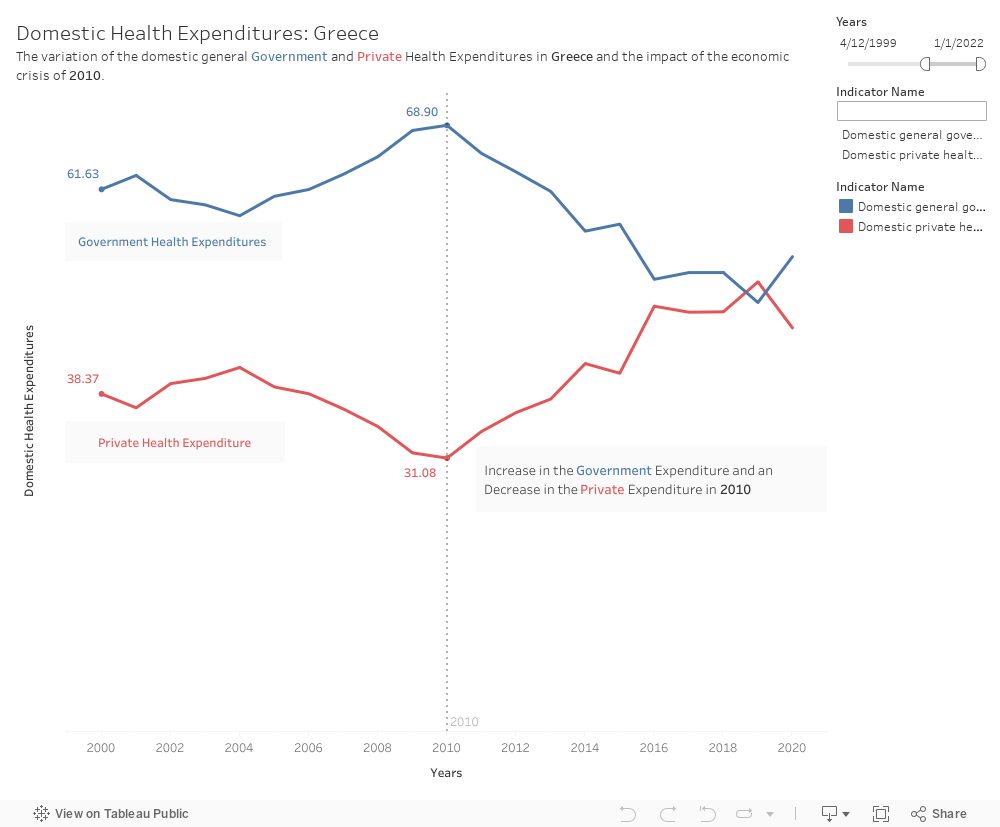
Greece’s Response in 2010: As the economic crisis unfolded in Greece, the government faced the daunting challenge of preserving essential public services, including healthcare. Despite severe austerity measures, Greece was able to maintain a relatively stable level of public health expenditure, thanks in part to support from the EU. The EU, in collaboration with the International Monetary Fund (IMF) and the European Central Bank (ECB), provided financial assistance and worked closely with Greek authorities to implement structural reforms.
In the tumultuous landscape of Greece’s economic crisis, the government, stood resilient in preserving public health expenditure due to the support of the EU. Aligned with SDG 3 (Good Health and Well-being) Greece’s commitment to maintaining health services during austerity was instrumental in ensuring equitable access to healthcare, mitigating potential disparities among its citizens.
Maintaining Public Health Expenditure: The EU support for Greece’s health sector included targeted funds, policy guidance, and technical expertise. Greece’s commitment to maintaining public health expenditure, even amid broader economic challenges, was seen as a strategic priority. The EU assistance helped Greece safeguard essential healthcare services, ensuring that the population continued to have access to medical care despite the economic downturn. Greece was able to increase its public health expenditures and decrease its private health expenditures even in light of the crisis.
Investment in Health Infrastructure: One key aspect of the EU support was the emphasis on investing in health infrastructure and promoting efficiency within the healthcare system. This approach aimed not only to address immediate needs but also to build a foundation for long-term sustainability. Greece utilized these funds to upgrade medical facilities, enhance healthcare delivery, and improve overall public health outcomes.
Lebanon:
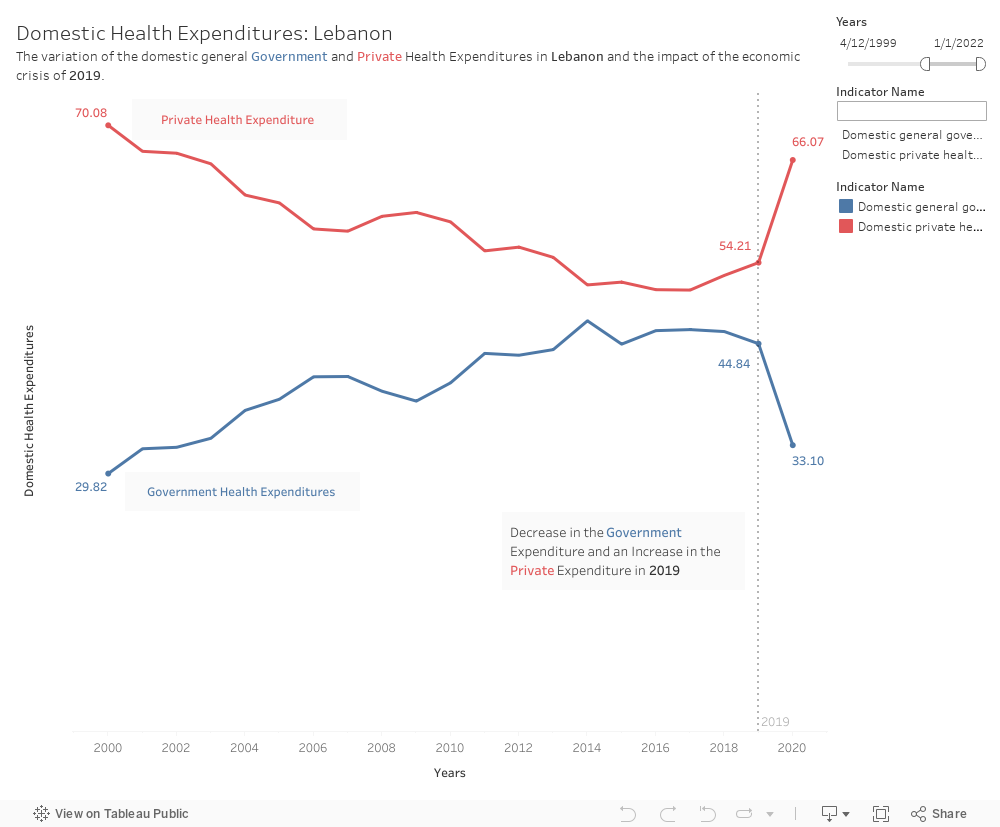
Lebanon’s Struggle in 2019: In contrast, Lebanon faced a more challenging situation in 2019. The absence of a supportive regional union akin to the EU left Lebanon with fewer external resources to combat its economic crisis. Rampant corruption, compounded by political instability, hindered effective governance and the ability to mobilize funds for public services.
Public Health Expenditure Dilemma: As Lebanon grappled with economic turmoil, the public health sector bore the brunt of budget cuts. Public health expenditure decreased, leaving the population vulnerable, particularly in a time when healthcare needs were escalating with the rise of COVID 19. The lack of external support and a fragmented political landscape hindered Lebanon’s capacity to protect its citizens’ health. The economic crisis of 2019 prevented Lebanon from safeguarding the situation of its citizens. The public health expenditure decreased significantly and the private health expenditure increased which left citizens to bear the heavy load of the crisis.
Impact on Healthcare Accessibility: With decreased public health spending, the burden on private healthcare providers increased. Private health expenditure rose as individuals sought alternatives to strained public services. The divide in healthcare accessibility deepened, disproportionately affecting the most vulnerable populations who lacked the means to access private healthcare.
The divergent paths of Greece and Lebanon underscore the critical role of external support during economic crises. Greece’s ability to maintain a relatively stable level of public health expenditure with the assistance of the EU highlights the importance of collaborative efforts and financial support in times of crisis. In contrast, Lebanon’s struggle to secure external aid resulted in a significant impact on public health services. This tale serves as a reminder that international cooperation and support can play a pivotal role in mitigating the human costs of economic downturns, particularly in the realm of healthcare.
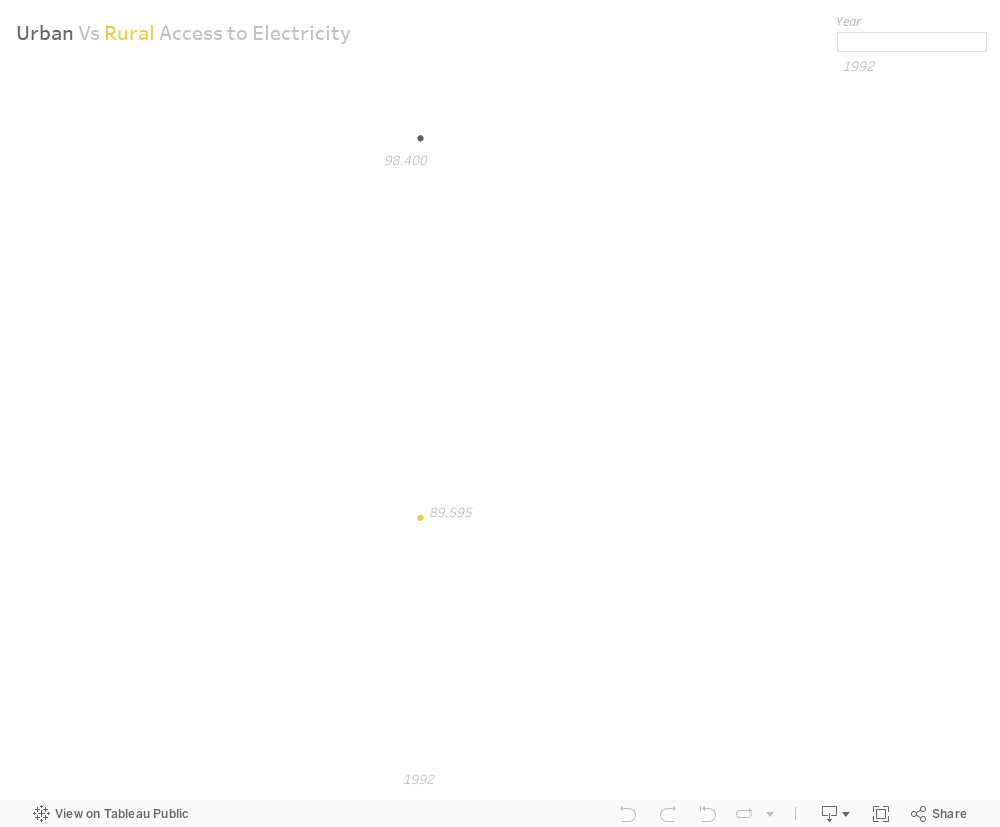
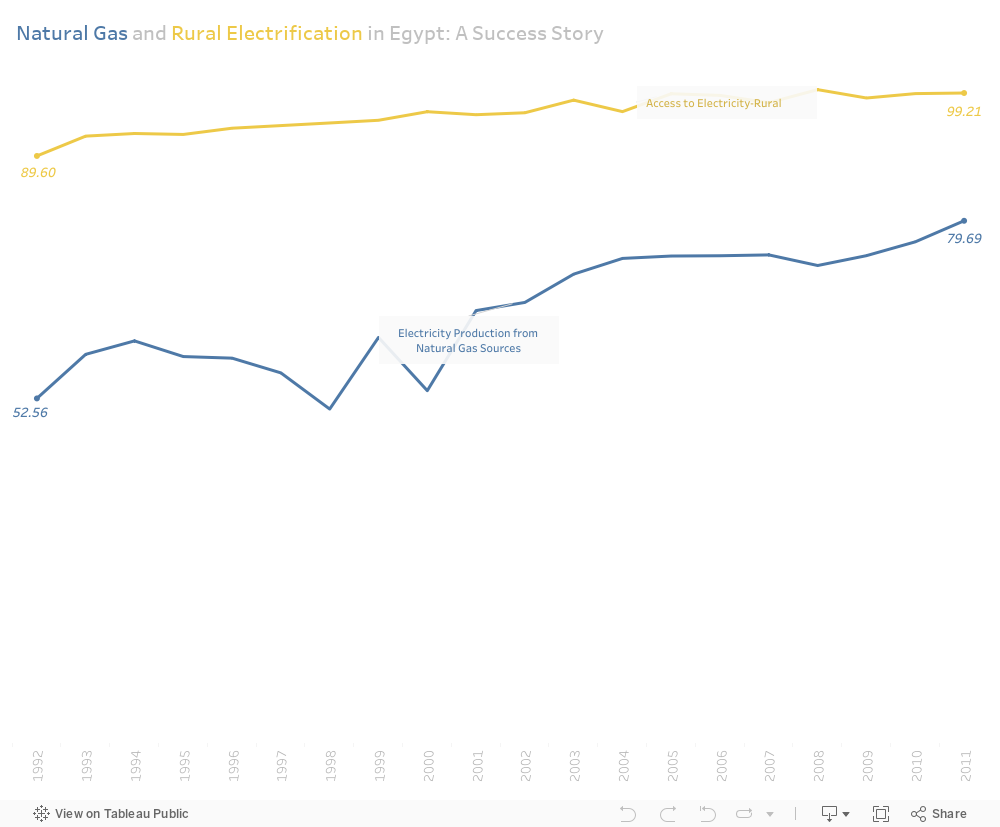
“Electricity is more than just a source of power for homes; it symbolizes hope and progress. However, this promise often goes unrealized for millions in rural areas around the globe. Egypt’s quest for energy equality—a story that started with challenges in 1992, the rise of a solution that not only brought electricity to villages but also changed lives.”
In 1992, Egypt faced a significant energy challenge with urban electrification at 98.4% and rural access lagging at 89.6%.
This disparity raised concerns about the inclusivity of the energy infrastructure and the well-being of rural communities.
A Greener, Cheaper, Overall Better Solution Emerges:
To tackle this formidable challenge, the proposed solution involved harnessing Egypt’s abundant natural gas resources. Natural gas, renowned for its cleaner and more sustainable attributes, emerged as a beacon of hope. The goal was not only to cater to escalating urban demands but to extend the benefits to long-overlooked rural areas, creating a more inclusive and environmentally friendly energy landscape. Additionally, natural gas offered economic advantages, being both cheaper and easier to remote in rural regions compared to traditional energy sources. This made it an ideal solution for bridging the energy divide and ensuring equitable access to electricity across Egypt.
Success Unveiled:
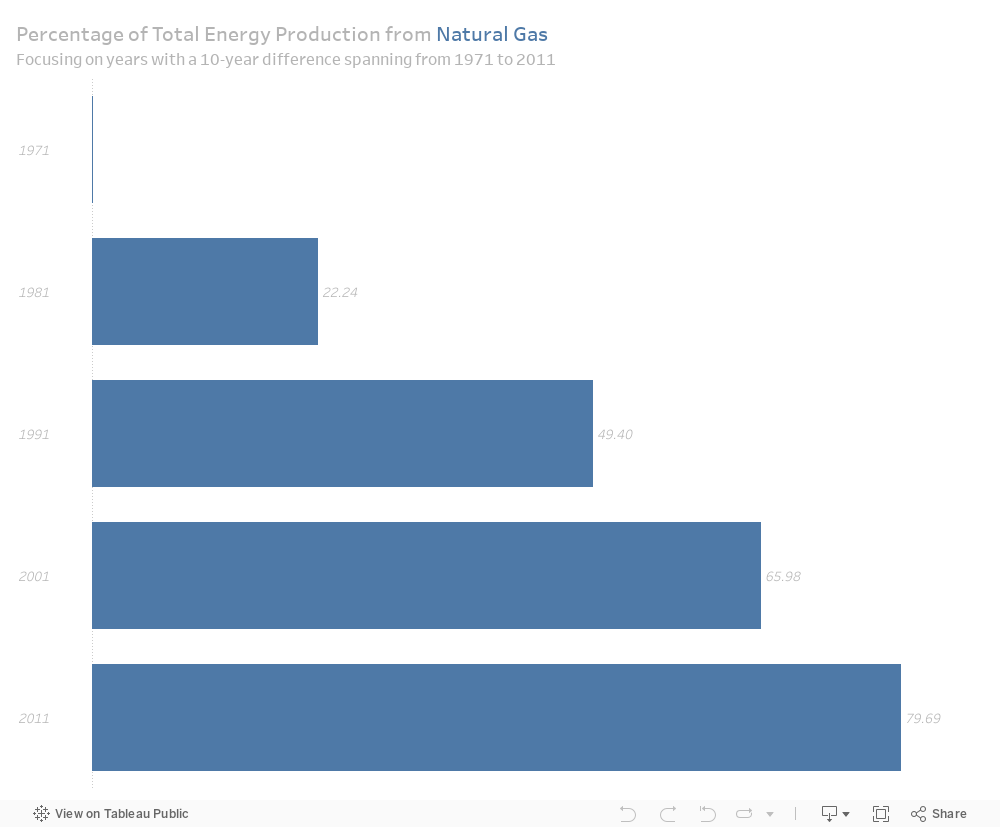
Natural gas production experienced substantial growth over the years, having a major role in impacting the construction of a resilient and accessible energy infrastructure. this economic viability made it an attractive solution for bridging the energy gap and ensuring equitable access to electricity across Egypt. This success wasn’t confined to urban centers but rippled out to rural communities, ensuring that the positive impact of electrification reached every corner of the nation.
The percentage of natural gas production witnessed remarkable growth over 10-year intervals, rising from nearly zero in 1971 to around 80% in 2011.
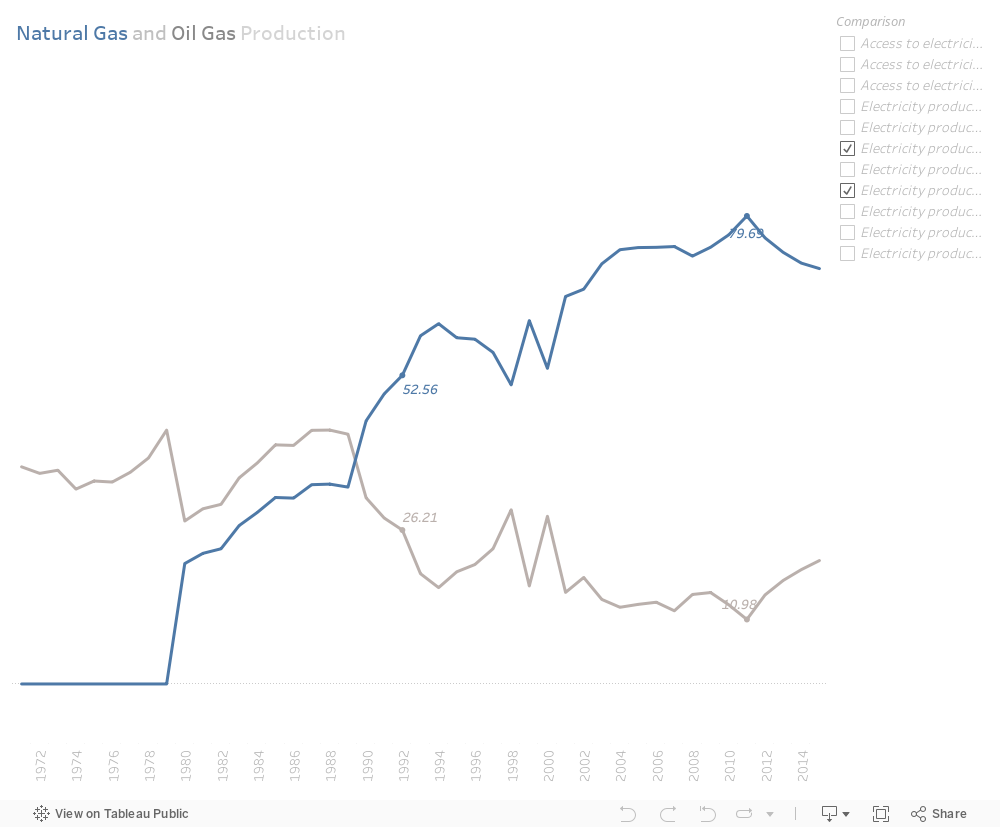
Symmetry, With Oil Sources:
There the growth of natural gas production aligns symmetrically with the decline in oil sources production. This visual harmony provides irrefutable evidence that the strategic integration of natural gas was not only effective but also instrumental in reducing dependence on less sustainable energy sources.
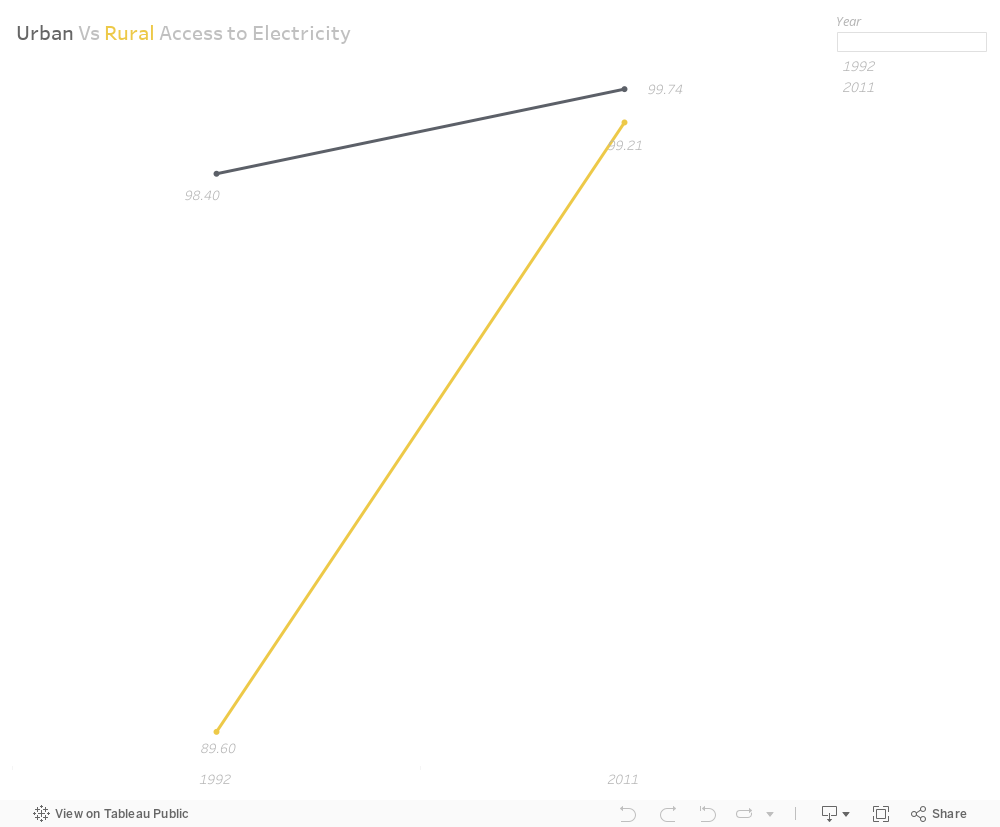
Fast forward to 2011:
Urban access surged to an impressive 99.74%, the most notable achievement was the substantial growth in rural electrification, which improved significantly (more than 10%) to reach 99.2%.
This visual representation underscores the remarkable progress in bringing electricity to rural areas, signaling a successful effort to bridge the gap.
Rural Electrification Triumphs:
The real triumph lies in the positive outcomes witnessed in rural electrification, as exemplified in the narrative of “Natural Gas and Rural Electrification.”
The integration of natural gas into the energy mixes catapulted Egypt into a new era—a landscape marked by balance, sustainability, and a profound impact on rural communities. The findings underscore the success of aligning energy production with both environmental and social imperatives.
In a world teeming with progress, one persistent challenge darkens our collective horizon – the rising specter of suicide. Behind the cold statistics lie countless untold stories of despair, each one a testament to the urgent need for a compassionate and effective response. Let us delve into the stark realities that underscore the gravity of this issue.
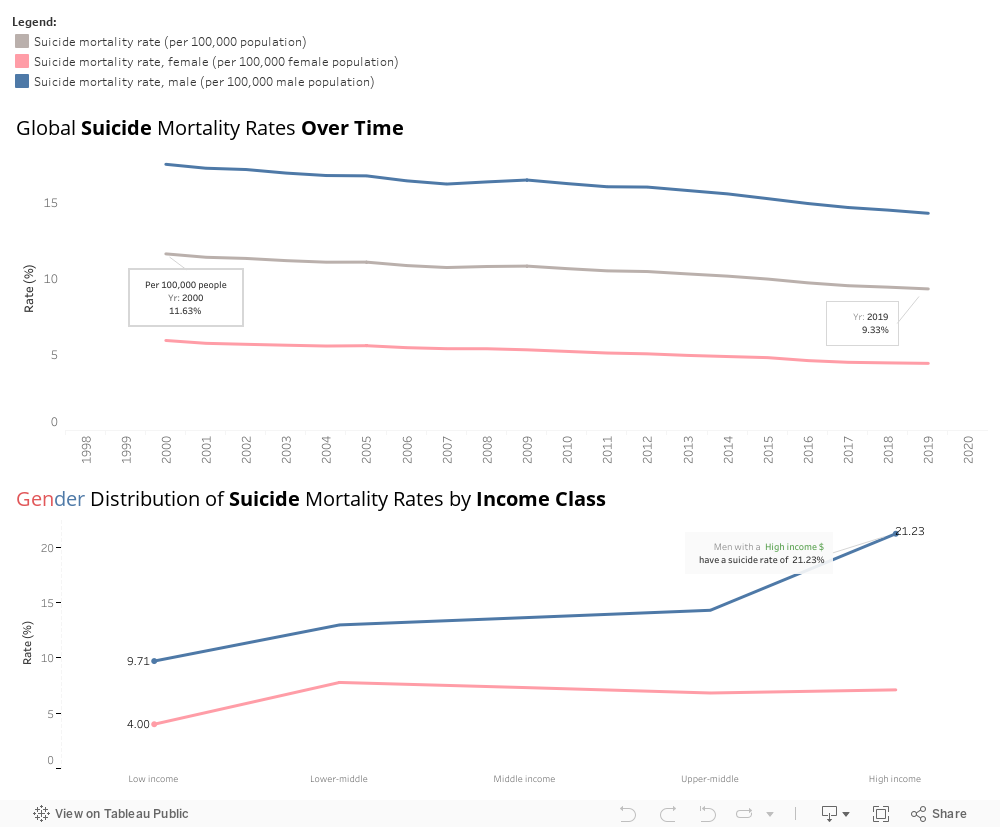
The global landscape of suicide mortality rates is a sobering tableau. Over the years, the data reveals a consistent gender disparity, with male suicide rates consistently surpassing those of females. Between 2000 and 2019, the male suicide rate remained at an alarming average of 16.075%, overshadowing the female rate. While there has been a slight decrease in the overall rate, from 11.63% in 2000 to 9.33% in 2019, the persistence of high numbers and occasional spikes, like the one in 2013, signals an urgent need for intervention.
Economic disparities exacerbate the issue, as revealed by the Gender Distribution of Suicide Mortality Rates by Income Class. Notably, those with low income levels exhibit lower suicide rates (9.71% for males and 4% for females), hinting at a potential link between financial struggle and mental health. Paradoxically, the highest suicide rate is observed among high-income males, reaching a staggering 21.23%. The reasons behind this economic divergence merit careful consideration.
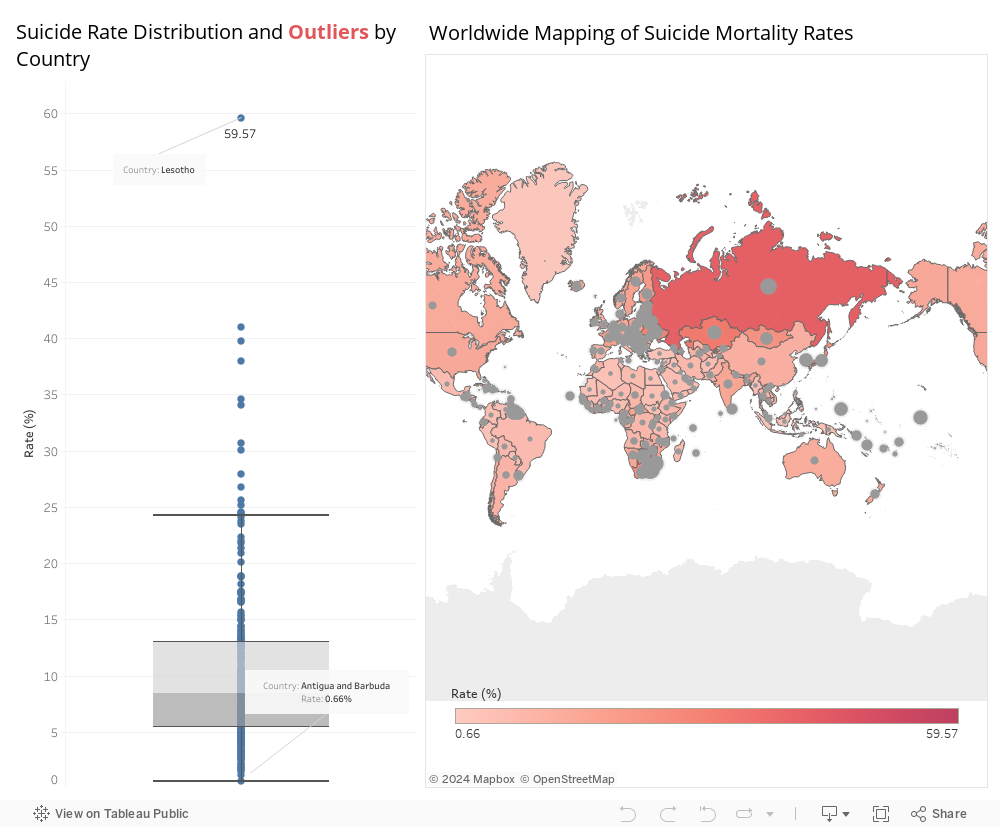
Zooming in on a country-by-country perspective, certain nations emerge as outliers, bearing the weight of exceptionally high suicide rates. Lesotho, Eswatini, the Russian Federation, Guyana, Kazakhstan, Kiribati, Ukraine, South Korea, Botswana, Latvia, and Hungary are among the nations grappling with disproportionately high suicide rates. Identifying patterns within these outliers offers crucial insights into potential factors contributing to the crisis.
We should collaborate on comprehensive mental health education programs to destigmatize mental health issues and foster a culture of open communication. Developing targeted support systems for individuals facing economic challenges will address the intricate relationship between financial struggles and mental health. Strengthening community support systems to identify and aid individuals at risk ensures that no one is left to battle their demons alone.
Comprehensive Strategies for Mental Health Advocacy against Suicide could be the following:
Collaborate with educational institutions to integrate mental health education into curricula, focusing on destigmatization, early detection, and coping mechanisms.
Implement awareness campaigns to reach a broader audience and enhance understanding of mental health issues.
Establish programs offering financial counseling, employment assistance, and mental health resources tailored to different income groups.
Foster partnerships with businesses to create inclusive work environments that prioritize employee well-being.
Develop community-based mental health initiatives, including support groups, helplines, and outreach programs.
Encourage local leaders to champion mental health awareness and facilitate resources at the grassroots level, strengthening community outreach efforts.
In conclusion, conducting pilot programs in select regions to assess the effectiveness of the proposed solutions is a necessary step. Moreover, utilizing quantitative and qualitative metrics, such as changes in suicide rates, public awareness, and community engagement, will help evaluate the impact of implementing these measures.
Findings/Recommendations:
Upon validation, refining and scaling successful programs for broader implementation is the next logical step. Advocating for policy changes that prioritize mental health and allocate resources to address the multifaceted challenges contributing to the global suicide crisis is crucial. Remember, breaking the chains requires a collective effort – a united front against the darkness that shrouds the lives of those grappling with the heavy burden of despair.
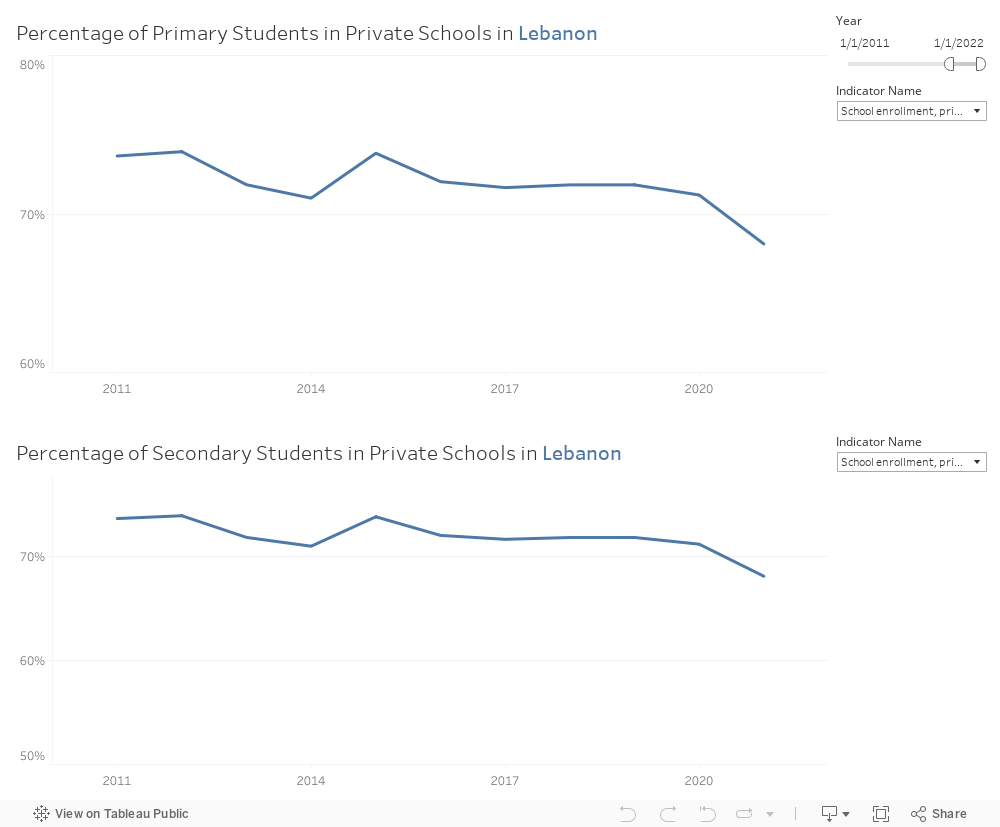
Lebanon’s public education sector has grappled with numerous challenges in recent years, such as a shortage of spots in public schools, strikes by primary and secondary teachers, and various other issues. As a previous student in the public sector, STRIKE! was the most common act I encountered from my teachers. A lot of strikes and movements were organized by teachers, asking for their rights, increased wages, etc.. This was a great disabler for an efficient learning journey, where stability, the most important aspect was absent. Such a state deprived students, in one way or another, of having access to free and inclusive educational institutions/schools. For that reason, a comprehensive study I conducted revealed that a significant number of students have turned to private schools as an alternative, highlighting a critical problem in achieving the Sustainable Development Goal (SDG) of providing quality and inclusive education for all students.
.
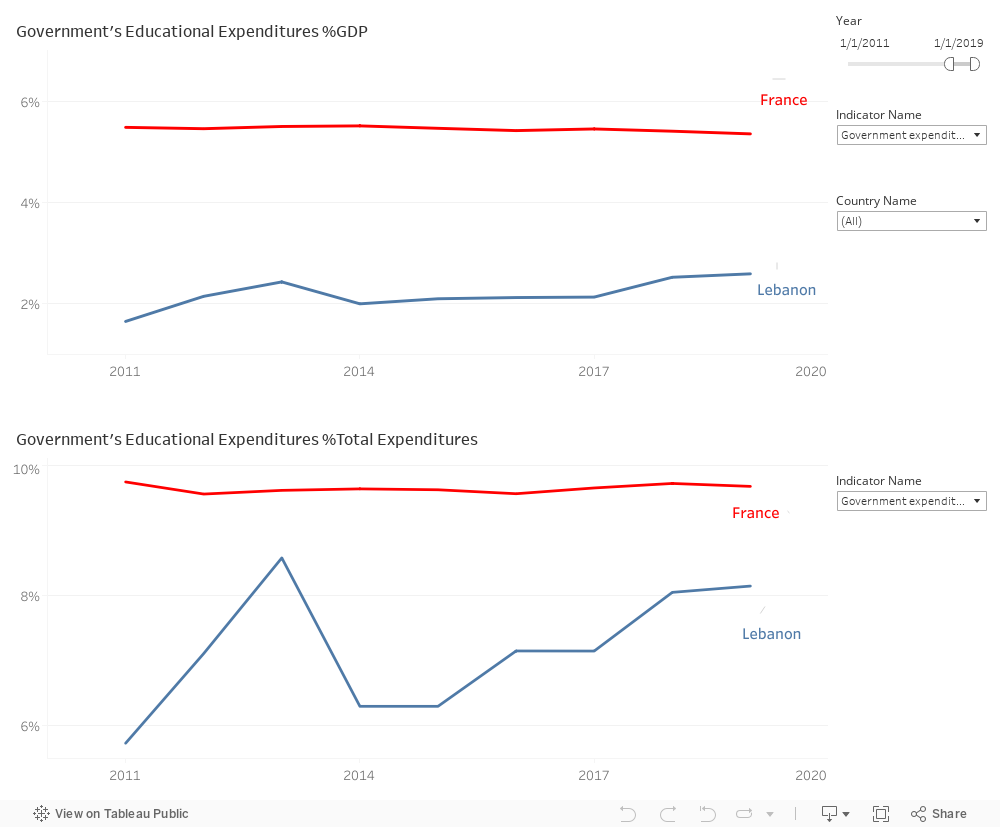
To address the issue of the lack of educational opportunities in public schools, which should be guaranteed by the government, as the 4th goal of SDG states, an examination of Lebanon’s education expenditure as a percentage of GDP was undertaken, where reflects the amount of money the government spends on education, in addition to another factor, which is the percentage of government’s expenditures on education as a percentage of total expenditures, These 2 metrics are then considered particularly in comparison to France, given Lebanon’s adherence to the French Educational System. The analysis of these two metrics exposed a disparity, with Lebanon’s current education expenditure as a percentage of GDP having risen since 2019 due to the economic crisis, reaching 2% in 2022, compared to France’s 6%. Although Lebanon fares well in terms of the percentage of education expenditures compared to other sectors, with a steady increase since 2014, reaching nearly 8% in 2020 in contrast to France’s 10%, the gap in GDP percentage remains concerning.
In conclusion, addressing this issue requires recommending an augmented budget for Lebanon’s educational sector. Ideally, a tripling of the budget over the next decade is proposed. This increase could be implemented gradually, but decisive action must be taken to ensure progress towards the SDG of providing quality and inclusive education for all Lebanese students.