This does not start with a funny caption or a happy anecdote, but I assure you it’s an important topic and it touches the lives of everyone. This is Tarek Moukalled, and I hope that by the end of this session you can see the light at the end of the tunnel for patients in Lebanon.
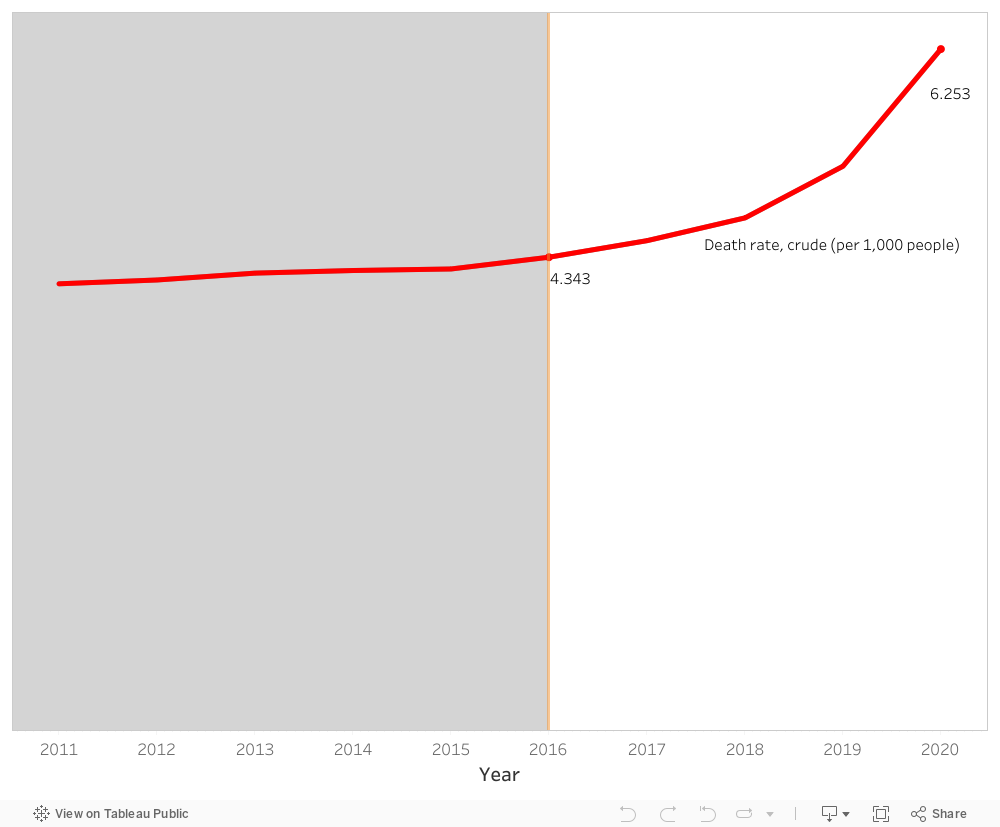
Our story begins with rather an unfortunate observation. Patients in Lebanon are dying. As a matter of fact, the death rate has increased from 4.34 deaths in 2016 to 6.25 deaths in 2020 per 1,000 persons. That is drastic and an alarming increase of approximately 44 % during a span of 5 years. But why?
A close inspection of the healthcare expenditure per capita during the suggested years shows a considerable increase from 648 USD to 995 USD. Furthermore, the % expenditure of GDP on healthcare in Lebanon also shows a consistent trend of a little less than 8 % across the same years. So, things should be fine, if not better! Yet unfortunately, this is not the case.
It appears the Lebanese people have been taking things into their hands. With the economic recession and the subsequent governmental bankruptcy, GDP decreased from ~ 51.1 billion USD in 2016 to 31.7 billion USD in 2020. This led to the fact that the Lebanese people have been paying more and more from their own pockets for healthcare reaching a whopping 44.2 % of healthcare expenditure in 2020.
Comparing the above results with the healthcare sector of a different country that shares similar demographics and healthcare expenditure with Lebanon would help with the context and the subsequent validation of the proposed solution, the light at the end of the tunnel. Remember?
With a similar % expenditure of GDP on healthcare (~ 7.5 %) and a little lower starting point in death rate of 3.16 per 1,000 persons, Jordan’s death rate in 2020 reaches 3.47 per 1,000 persons. The healthcare expenditure per capita in Jordan is consistently way lower than that of Lebanon. The % of out-of-pocket expenditure on healthcare is also steady and lower than that of Lebanon. As to the GDP, it starts lower than Lebanon in 2016 at ~ 39.9 billion USD and ends higher than Lebanon at 43.6 billion USD. As such, the main considerable deviation between both countries is the GDP amount. For that matter, it’s important to note that economies and healthcare sectors grow through expenditure rather than stagnation or restriction.
The increase in the share of health expenditure as part of GDP will have positive results on both short-term and long-term.
Enhanced Healthcare Quality
Faster Healthcare Response
Improved Patient Health Outcome
Decreased Death Rate
Target for Healthcare Tourism
With that, it is imperative to urge whoever who is responsible to proceed with the increase in healthcare expenditure for the sake of our patients and our future.
In the wake of economic crises that shook nations, Lebanon in 2019 and Greece in 2010 faced turbulent times. Both crises were rooted in corruption, leading to drastic declines in GDP growth. However, the divergent paths they took in managing their public health expenditures reflected the crucial role of external support, particularly from the European Union (EU), in shaping their healthcare resilience. The following graph depicts the impact of each economic crisis on the growth of the GDP for each country.
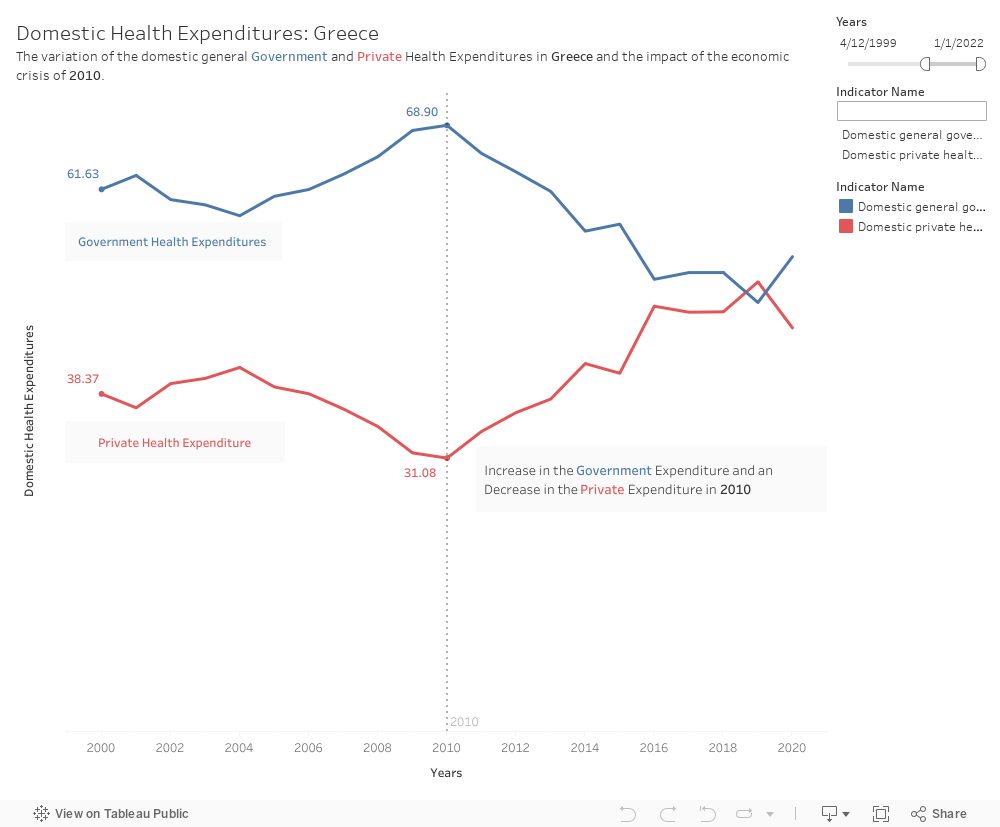
Greece:
Greece’s Response in 2010: As the economic crisis unfolded in Greece, the government faced the daunting challenge of preserving essential public services, including healthcare. Despite severe austerity measures, Greece was able to maintain a relatively stable level of public health expenditure, thanks in part to support from the EU. The EU, in collaboration with the International Monetary Fund (IMF) and the European Central Bank (ECB), provided financial assistance and worked closely with Greek authorities to implement structural reforms.
In the tumultuous landscape of Greece’s economic crisis, the government, stood resilient in preserving public health expenditure due to the support of the EU. Aligned with SDG 3 (Good Health and Well-being) Greece’s commitment to maintaining health services during austerity was instrumental in ensuring equitable access to healthcare, mitigating potential disparities among its citizens.
Maintaining Public Health Expenditure: The EU support for Greece’s health sector included targeted funds, policy guidance, and technical expertise. Greece’s commitment to maintaining public health expenditure, even amid broader economic challenges, was seen as a strategic priority. The EU assistance helped Greece safeguard essential healthcare services, ensuring that the population continued to have access to medical care despite the economic downturn. Greece was able to increase its public health expenditures and decrease its private health expenditures even in light of the crisis.
Investment in Health Infrastructure: One key aspect of the EU support was the emphasis on investing in health infrastructure and promoting efficiency within the healthcare system. This approach aimed not only to address immediate needs but also to build a foundation for long-term sustainability. Greece utilized these funds to upgrade medical facilities, enhance healthcare delivery, and improve overall public health outcomes.
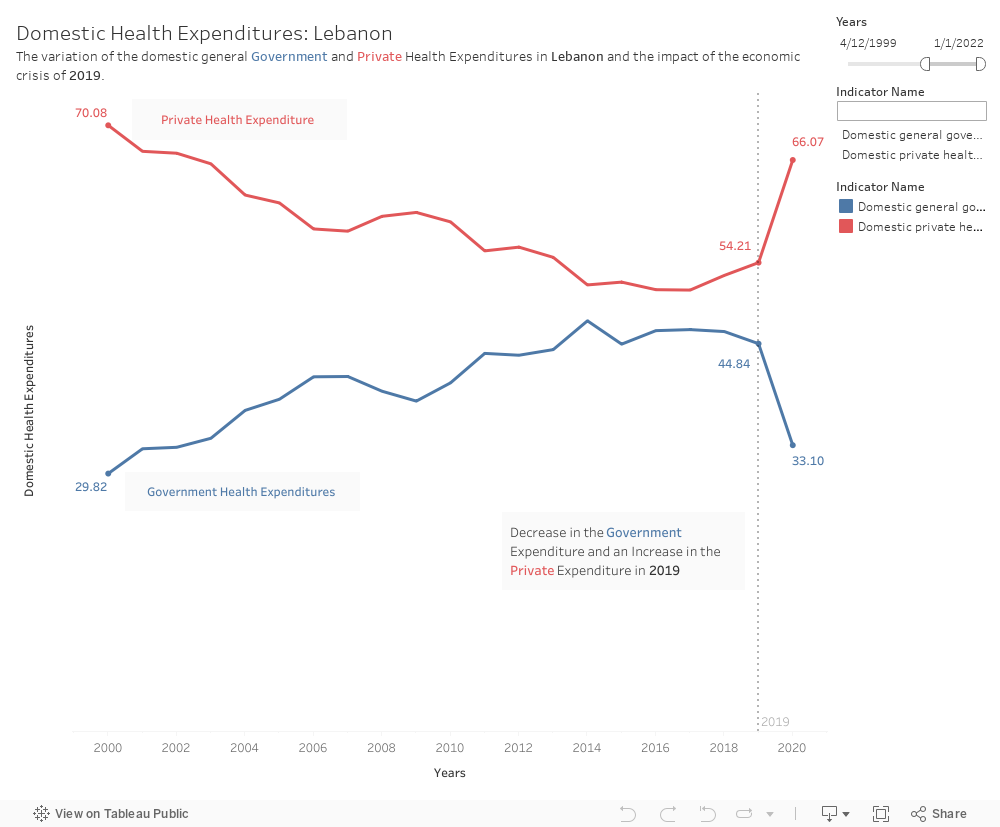
Lebanon:
Lebanon’s Struggle in 2019: In contrast, Lebanon faced a more challenging situation in 2019. The absence of a supportive regional union akin to the EU left Lebanon with fewer external resources to combat its economic crisis. Rampant corruption, compounded by political instability, hindered effective governance and the ability to mobilize funds for public services.
Public Health Expenditure Dilemma: As Lebanon grappled with economic turmoil, the public health sector bore the brunt of budget cuts. Public health expenditure decreased, leaving the population vulnerable, particularly in a time when healthcare needs were escalating with the rise of COVID 19. The lack of external support and a fragmented political landscape hindered Lebanon’s capacity to protect its citizens’ health. The economic crisis of 2019 prevented Lebanon from safeguarding the situation of its citizens. The public health expenditure decreased significantly and the private health expenditure increased which left citizens to bear the heavy load of the crisis.
Impact on Healthcare Accessibility: With decreased public health spending, the burden on private healthcare providers increased. Private health expenditure rose as individuals sought alternatives to strained public services. The divide in healthcare accessibility deepened, disproportionately affecting the most vulnerable populations who lacked the means to access private healthcare.
The divergent paths of Greece and Lebanon underscore the critical role of external support during economic crises. Greece’s ability to maintain a relatively stable level of public health expenditure with the assistance of the EU highlights the importance of collaborative efforts and financial support in times of crisis. In contrast, Lebanon’s struggle to secure external aid resulted in a significant impact on public health services. This tale serves as a reminder that international cooperation and support can play a pivotal role in mitigating the human costs of economic downturns, particularly in the realm of healthcare.