
Teta Salma lives in a small village in the Hermel District. The nearest clinic is far from her home and opens on an unpredictable schedule, so routine tests are rarely part of her life. She often feels tired but assumes it is simply age catching up with her. During a visit to her daughter in Mount Lebanon, she took her to a nearby medical center for a simple checkup. That day she learned she had diabetes. The condition had been part of her life for years. It had only been discovered because she finally had access.
Her experience reflects something that appears across Lebanon when we look at the data. Using the Health Status 2023 and Health Resources 2023 datasets from PKGCube, I compared reported chronic disease cases with the number of healthcare facilities available in each governorate and district. I combined hypertension, cardiovascular disease and diabetes into one chronic disease measure. I then compared these counts with the number of care centers and first aid centers in each region:
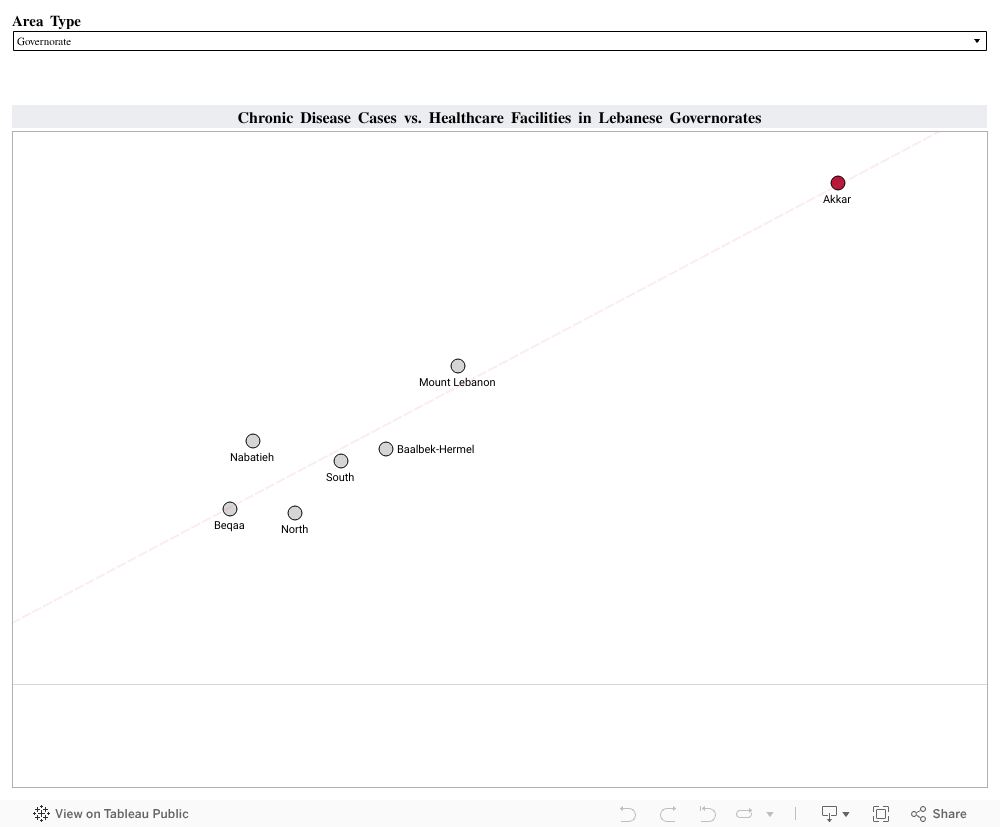
The visualization revealed a clear pattern: Regions with stronger reach and more places to get a routine check reported higher counts of chronic disease. Akkar stands out with 390 chronic disease cases and 126 healthcare facilities. Mount Lebanon and Baalbek Hermel show a similar alignment. Areas with limited reach, such as Hermel or the Western Beqaa, showed much lower numbers.
These lower numbers do not necessarily reflect lower illness. They reflect reduced visibility. When people cannot reach a clinic easily, fewer conditions are recorded and many remain unnoticed until symptoms become harder to ignore.
To understand how better reach affects health data, I looked at the experience of Thailand. The country expanded primary care and community screening through its Universal Health Coverage program. Once routine checks became easier to access, more cases of hypertension and diabetes were identified, especially in rural areas. Detection of hypertension increased from 48.9 percent in 2016 to 53.3 percent in 2019, and diabetes detection rose from 67.4 percent to 74.7 percent during the same period. These changes showed how wider access can reveal conditions that were present long before.
This is similar to what we see in Lebanon. When people have access, more of the country’s true chronic disease burden becomes visible. When access is limited, the data looks lighter than reality.
A practical next step for Lebanon is to expand routine screening in districts with fewer facilities. Mobile clinics, community testing days and partnerships with universities or NGOs can bring basic checks closer to the communities that need them. Improved digital record systems can also help track early diagnoses more accurately. Monitoring places like Hermel, Bsharri or the Western Beqaa can show if these efforts are working.
Healthcare access shapes what we know about people’s health. Strengthening that access gives families the chance to understand their conditions earlier and manage them with clarity. It also brings us back to people like Teta Salma. Her diabetes did not begin the day she was screened. It became visible because she finally reached a place where someone could help her.
Supporting more communities in this way can bring hidden conditions to light and build healthier lives across Lebanon.
0 Comments