
In Heart Attacks, Every Minute Lost Reduces Survival
Heart attacks don’t negotiate. Once symptoms start, the countdown begins and survival depends on how fast a patient reaches a hospital that can intervene. This makes geography a health factor.
In Lebanon, where hospitals are not evenly distributed across districts, access time can vary sharply from one place to another. The question isn’t only “how many heart cases do we have?” but also “how close is care when those cases happen?”
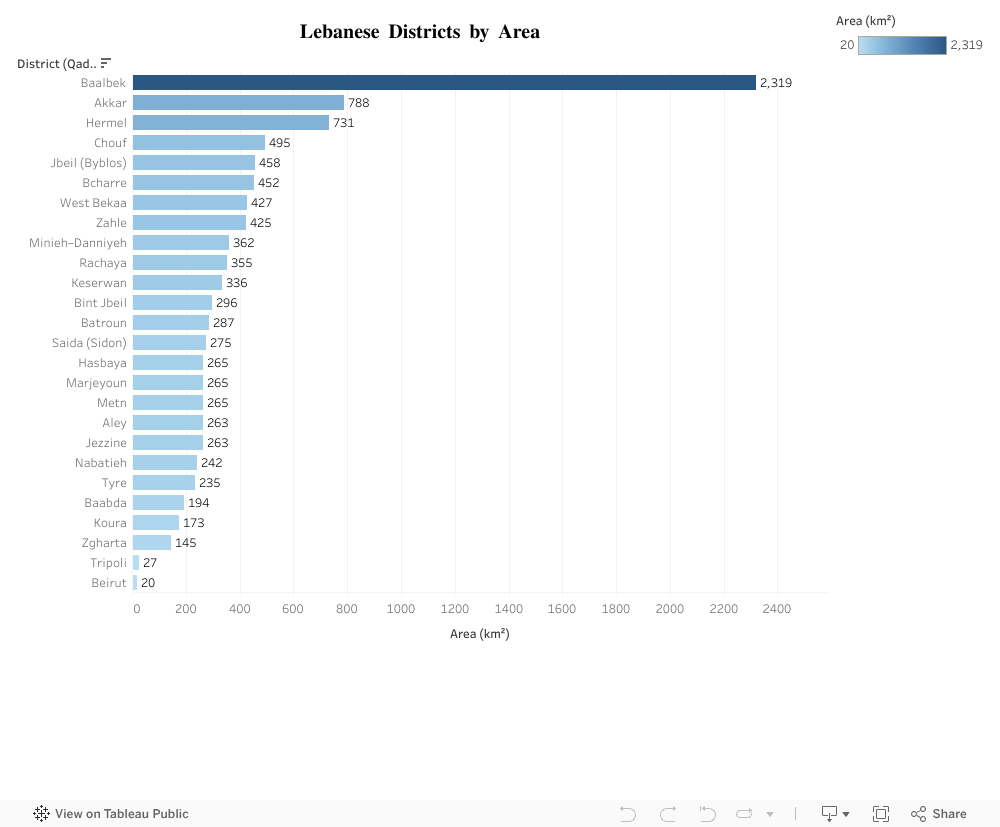
Akkar vs. Baabda: A District Size Contrast That Matters
Akkar and Baabda illustrate Lebanon’s geographic contrasts clearly. Akkar spans 788 km², making it one of the largest districts in the country, with wide and spread out communities. Baabda, by comparison, covers just 194 km² nearly four times smaller.
This difference isn’t just a cartographic detail; it fundamentally shapes residents’ access to services. In a district as large as Akkar, simply reaching a hospital can take significantly more time, while Baabda’s compact size naturally supports quicker, more concentrated access to care.
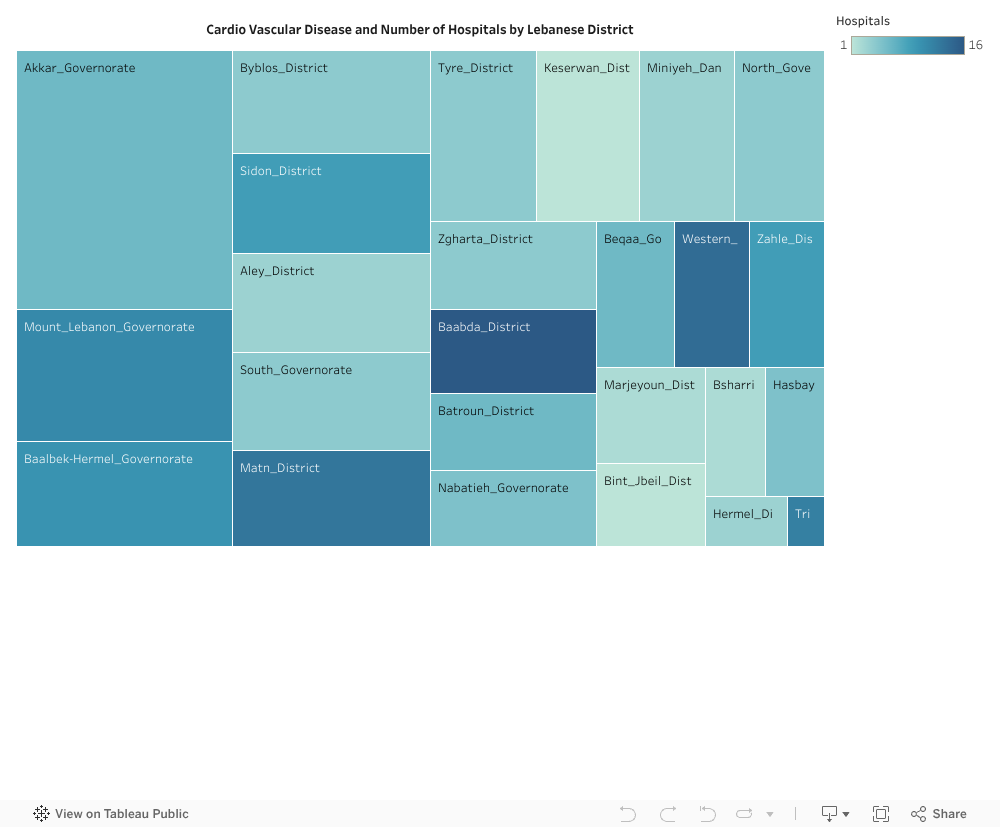
Mismatch between burden and capacity
Akkar also shows a high cardiovascular case load
In other words:
- Big territory → longer distances by default
- Low hospital density → fewer nearby entry points for emergency care
- High cardiovascular cases → more people needing urgent access
That combination is a red flag. It implies that when heart attacks strike in Akkar, residents are more likely to face delayed arrival to care compared to smaller, better served districts.
What could realistically improve this?
This isn’t about building a hospital in every village. It’s about optimizing emergency reach. Lebanon already has health infrastructure, the strategic gap is spatial coverage and speed.
A practical way forward is to reduce time to care in high burden, low coverage districts through targeted interventions such as:
- Upgrading/expanding emergency-capable units in under-served districts
- Deploying advanced ambulance hubs positioned for maximum coverage
- Formalizing rapid transfer pathways to the nearest cardiac-capable hospital
The goal is simple: even if a hospital isn’t next door, the system should behave like it is by cutting delays.
How to prioritize smartly?
The visuals naturally suggest a prioritization logic:
- Identify districts with high cardiovascular cases (large bars / darker heat).
- Among them, flag those with low hospital density (lighter color).
- Cross-check physical area (larger districts imply longer response routes).
Districts like Akkar fall into the high-priority quadrant: large area, high burden, low coverage. These are the districts where a marginal improvement in access time could prevent disproportionately more deaths. That’s high ROI health policy.
Align capacity with need
If we reduce time in districts like Akkar, through more emergency nodes, better equipped local units, or faster transfer networks, we align capacity with need without requiring unrealistic nationwide hospital expansion.
Next Steps?
Lebanon should treat emergency cardiac access as a geographic equity issue. Health planning must go beyond counting hospitals, it should measure how fast people can reach lifesaving care, especially in high burden districts.
Because in a heart attack, there’s no such thing as an average patient. There’s only the patient who needs help now, and whether help is close enough to arrive in time.
0 Comments