DATA MANAGEMENT UNIT
Data management plays a major role in collecting data on diagnostic findings, treatment, and follow up in the cancer database through the recently developed E-forms, adopted from the latest American Society of Clinical Oncology (ASCO) cancer-specific forms.
The data management team generates quarterly/yearly reports to support decision-making, manages clinical trials, prospective and retrospective studies and keeps record of ongoing studies. The data management team works closely with research fellows, Clinical research associates (CROs), decision resources team, and coordinates with the electronic medical record health system – EPIC – team to update the Oncology database and the Tumor registry.
ONCOLOGY DATABASE
The volume of patients treated and diagnosed with cancer over the past decade has been continuously increasing, in addition, the tumor registry information was restricted to minimal demographics and tumor location and morphology. This information was used to supply the National cancer registry with the AUBMC incidence rates, and to identify specific cancer populations for AUBMC researchers. Following the rapid innovations in cancer research, the need for a comprehensive tool was crucial to combine additional treatment and follow up information to supply and support our team. The Oncology database was essential for researchers to collaborate and combine basic, translational, and clinical research to explore ways to prevent, control, and treat cancer.
The oncology database launched in October 2014 and initially focused on three cancer sites: Breast, colon and prostate. A year later, lung cancer was introduced.
This method of data collection stores data on an online internal system to secure a comprehensive database on cancer cases. Using electronic E-forms, the Data Management has expanded the current cancer data quality in Lebanon by gathering detailed data when the patient is admitted.
Data collected includes demographics, consents, pathology and blood tests, treatment, surgical procedures, imaging, treatments, medications, in addition to follow up information and medical outcomes. Unlike the tumor registry this database includes treatment details, and constant updates on patients’ therapy upon each visit. As patients are pre-consented upon their admission, subsequent follow-ups are made possible through contacting the patients and collecting medical outcome information.
The oncology database’s forthcoming plan is to add non-solid tumors that include hematologic and lymphatic tumors to the database.
The E-forms have been integrated within the new AUBMC EPIC electronic health system to capture data directly from the new system and minimize time and effort collecting this information. A prompting message now secures patient consent to be contacted for future research participation.
TUMOR REGISTRY
HISTORY
The tumor registry has been a fundamental part of Oncology since its initiation in 1983. an essential part of the data management in the clinical research unit. Its primary function was to maintain a registry of all cancer cases visiting AUBMC. Clinical and pathological characteristics of cancer patients were collected continuously and systematically from various data sources and stored in the cancer registry database.
The registry analyzed and interpreted data periodically and provided information on the incidence and characteristics of specific cancers in various segments of the resident population and on variations in incidence in time. Such information was the primary resource not only for epidemiological research on cancer determinants, but also for planning and evaluating health services for the prevention, diagnosis and treatment of the disease.
The Tumor registry completed in 2018 its 35 years of continuous data collection. The tumor registry is no longer serving its initial operation, since the beginning of 2019, all cases collected in the Tumor registry since 1983 serve now as an archive.
After the implementation of EPIC, a set of automated reports were tailored to be run monthly in order to produce needed statistics of current patient volume, diagnoses and other patient related demographic information.
The data is now secured, locked, and later accessible for historical data and assessment. The Tumor registry data continues, however, to provide the Ministry of public health with the number of cancer cases for the remaining years in the National cancer registry until 2018.
The total number of cancer patients enrolled at NKBCI Tumor Registry since 1983 till October 2018 is 50,895
ROLE
Epidemiological research, based on comprehensive cancer registration, was the most valid and efficient way to plan and evaluate all aspects of cancer control. Cancer registries have an important supportive role in the care of cancer patients by assisting clinicians in the follow-up of their cases and by providing statistical data on the results of therapy.
The cancer registry in AUBMC collected data from pathology, radiation oncology, hematology and dermatology departments. The data management department used this data to generate annual reports that were discussed in the hospital committee on cancer, and were published on the Data management and clinical research unit. Moreover, the cancer registry played an essential role in retrospective data collection from medical records, and doctors’ clinics.
Our hospital-based cancer registry shared the data with the national registry on a yearly basis. The first national registry report was done for the year 2003, covering more than 90% of the cancer incidence in Lebanon in that year. Data was retrieved from independent and hospital-based pathology / hematology labs, and hospital based registries.
Our registry at AUBMC conformed to the norms set by the International Agency for Research on Cancer and the International Association of Cancer Registries which aims to provide guidelines on all aspects of cancer registration (IARC Scientific Publications No. 21). The importance of cancer registration in planning and evaluating cancer-related health services is dealt with in greater detail in the IARC monograph The Role of the Registry in Cancer Control (IARC Scientific Publications No. 66).
CANCERS IN LEBANON
- Here are some facts and figures on cancer in Lebanon based on the information collected by the data management unit:
Source: National Cancer Registry Data – Lebanese Ministry of Public Health (2015)
The average age of cancer incidence for AUBMC patients in 2018 was 56 years (+/-19.2 years).
Males represent 46% of the cases while 54% are females.
Cancer incidence in Lebanon and other neighboring countries was shown to be significantly lower than Western countries.
- For the year 2018-2019:
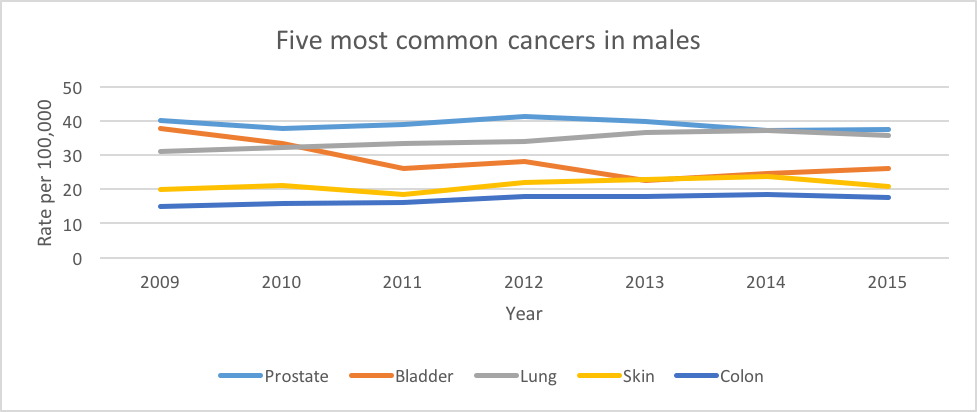
The most common cancers in men are:
- Prostate
- Bladder
- Lung
- non-Hodgkin lymphoma
- Colon
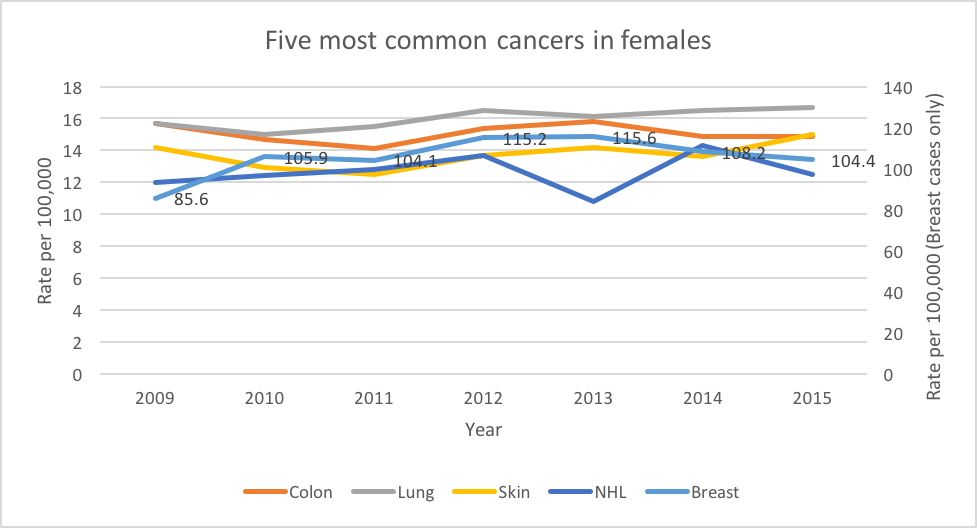
The most common cancers in women are:
- Breast
- Ovarian cancer
- non-Hodgkin lymphoma
- Lung
- Colon
- Facts on cancer incidence in Lebanon:
Tobacco smoking is a major cause of cancer in Lebanon. There has been an increase in smoking-related cancers, as tobacco smoking can cause cancer in almost any area of the body.
Lebanon has the highest rate of women smokers in Mediterranean countries, a rate that is increasing faster than any neighboring country.
Almost all smoking related cancers, especially lung and bladder, are increasing in Lebanon in both men and women.
The bladder cancer rate in Lebanon has been found to be among the highest in the world. This is directly associated with the dangerously high smoking rate.
- Cancer incidence trends in Lebanon over time:
Between 2003 and 2008, there has been an overall annual increase in cancer incidence for males and females of 4.5% and 5.4%, respectively.
Significant increases were observed for cancers of the liver and prostate for males, and for cancers of the liver, thyroid, and uterus for females
An aging population and a higher proportion of older people suggest further growth of cancer incidence in the future.
Smoking caused most cancer cases. Among many other cancers, lung cancer had the largest proportion attributable to smoking of around 75%.
Body Mass Index (BMI*) is expected to increase colorectal, liver and gastric cardia carcinoma specifically in males.
High physical activity has an average of 15% protection rate on cancer on colorectal cancer. Adhering minimally to a Mediterranean diet will affect gastric cancer incidence by 7%.
*BMI: BMI measures the amount of fat in the body based on height and weight: BMI = Body weight in kg / Height in meters x 2
REACH US
Ali Shamseddine, MD
Director Data Management Unit, Professor of Hematology – Oncology
At35@aub.edu.lb
Ext: 5150
Maya Charafeddine, MPH
Data Manager
mc16@aub.edu.lb
Ext: 5110
Monita Darazi, RN, MSN
Clinical trials Coordinator
Ma99@aub.edu.lb
Ext: 7804
Rachelle Bejjany, RN, MPH
Clinical trials Coordinator
Rb62@aub.edu.lb
Ext: 7803
QUICK LINKS
